Restless Limbs Sensorimotor Disorder
The purpose of this webpage is to provide an overview of my
observations and etiological hypotheses for the single disorder which
underlies the two diagnostic categories Restless Legs
Syndrome (RLS) and Periodic Limb Movement Disorder / Syndrome
(PLMD/S). In
addition to this, I discuss a variety of non-drug measures for
combating
this disorder.
If you are doctor, nurse, neurologist, neuroscientist, medical specialist or student, you might like to read the
shortest possible summary
of my observations and hypotheses which I wrote for a neurologist in
August 2012 and updated in February 2015. This contains some
updates, most recently in November 2017, which I have not yet made to the page you are reading now.
2020-05-30 update:
I haven't worked on RLSD for some
years, nor tried to keep up with the literature, This was
primarily because I found little new research concerning the spinal
cord - which is obviously where the pathology is located. It is
as if many neuroscientists are uninterested in the lowly spinal cord
when they could be working on
the brain.
However, please see this 2019 article, which reviews and discusses all
RLS/PLM work on spinal since the excellent 2000 article linked to
below:
#bara_jimenez Periodic
limb movements in sleep - State-dependent excitability of the spinal
flexor reflex
The 2019 review article is:
Much of what follows is novel and therefore likely to be controversial,
such as where in the body I believe the problem
occurs (the spinal cord); the biological processes which are involved;
and the
substances or environmental conditions which I believe are likely to
aggravate or diminish symptoms. Other statements are
in agreement with the widely-held views of medical researchers and
practitioners in this field, such as there being a single underlying
disorder to which the symptoms of both RLS and PLMD can be
traced, and the involvement of iron and dopamine in this disorder. Doctors prescribe the same treatments for both RLS and
PLMD. When these treatments are effective, they invariably
alleviate both
sets of
symptoms in the many patients who suffer both types of symptoms.
These new observations, etiological hypotheses and non-drug approaches
I am discussing have not yet been published in a peer-reviewed journal,
nor have they yet been the subject of widespread discussion by
established
researchers and clinicians. However, it is only since
September 2011 that I sent a paper (a 32-page PDF) documenting my ideas
and observations to 25 or so researchers in the RLS/PLMD
field. I am hoping to receive feedback from them.
If you are interested in RLS/PLMD research,
please let me know and I will send you a copy of the September 2011
document.
I suggest that the term Restless
Limbs Sensorimotor
Disorder (RLSD)
be used to refer to the single disorder which underlies these two
diagnostic categories. However, below, I use the acronyms RLS and PLMD,
because these are the currently accepted medical terms that are
familiar to people researching, treating, or suffering from this
disorder. Below, "RLS/PLMD" is my shorthand for this single
underlying condition. I hope that in the future, this will be
known as "RLSD".
This is a work in progress. The update history is: updates/ Please
let me know any corrections or suggestions.
Please be sure to read the DISCLAIMER regarding
health information at this site. I have no formal qualifications
and I am not a doctor. Even if I was a doctor, I have not
examined you!
To the index page of this site: ../
Contact details and copyright information: ../contact/
© 2011 to 2018 Robin Whittle Melbourne Australia
Last update except as noted above 6 November 2018.
Contents
| #intro
|
Introduction. |
#links
|
Links to other sites. |
| #summary |
Summary of my
new observations and etiological hypotheses. |
#help
|
Help for sufferers
and their carers - Non-drug techniques for combating RLS/PLMD.
01 - Self-diagnosis, with videos.
02 - Other patterns of movement which are
not RLS/PLMD.
03 - Ensure your iron levels are good.
04 - Do not drink coffee of any kind,
including decaf.
05 - Reduce or ideally eliminate your
consumption of caffeine.
06 - Dark chocolate and cocoa seems to
worsen or cause RLS/PLMD.
07 - Excessive salt seems to worsen or
cause RLS/PLMD.
08 - General nutrition, including Magnesium
and Calcium.
09 - Avoiding drugs which worsen the
condition.
10 - Sleeping position and keeping warm.
11 - Unusually high or low levels of
exercise.
12 - Protein meals and snacks.
13 - Tyrosine capsules or tablets.
14 - Percussive massage.
15 - Other factors and techniques.
|
#coffee
|
How
opioid receptor antagonists in all types of coffee might be expected to
increase the
severity of, or cause, RLS/PLMD symptoms. Also, some historical
notes on coffee, Thomas Willis writing in 1672 about coffee and about
what we
now know as RLS.
Also how some coffee drinkers find a cup of coffee stops symptoms and
helps them sleep - for an hour or so.
|
| #ownresearch |
The
nature of RLS/PLMD varies considerably between individuals. By
conducting your own research you can determine which treatments work
best for you.
|
On separate web
pages:
name-diag/
The DSM-5,
Diagnostic Criteria and a new name for Restless Legs Syndrome
Please see this page for my arguments for adopting
Restless Limbs Sensorimotor Disorder
in place of both RLS and PLMD, and to encompass less severe, but
still more widespread, symptoms concerning sleep disturbance. I
also argue against using family names to identify any pathological
condition.
The Restless Legs Foundation (
http://www.RLS.org)
and
the International Restless Legs Syndrome Study Group (
http://www.IRLSSG.org) have decided
to change the name of "Restless Legs Syndrome"
to "Willis-Ekbom Disease". Meanwhile, the American Psychiatric
Association are finalizing the DSM-5 to include diagnostic criteria of
"Restless Legs Syndrome", which was not in the DSM-IV. However,
the DSM does not cover
movement disorders. RLS/PLMD is a movement disorder.
It is not a sleep disorder, but it invariably disrupts sleep. It
is not a psychological or psychiatric disorder. Sufferers are
treated by their family doctor or neurologists - not by psychiatrists
or
psychotherapists.
Explanations of some neurological terms to help people understand the
summary below of my etiological hypotheses.
updates/
List of updates to
the pages in this RLSD section of the website.
[#intro]
Introduction
This section of the website outlines
new etiological hypotheses which I believe provide a good
explanation of the processes which underly the diagnostic categories
Restless Legs Syndrome (RLS) and Periodic Limb Movement
Disorder (PLMD). It also contains a list of non-drug
measures which I believe will help many people reduce or eliminate the
symptoms of the common - and for some people terribly disruptive -
neurological disorder which underlies these two diagnostic
categories.
The novel material here is based on observations and experiments
with
myself and my wife Tina, together with reports from friends who
have had some success with one or two of our suggested
techniques. Other RLS/PLMD sufferers with whom I have
corresponded or who have reported their experiences in web forums have
independently
discovered some of these techniques.
The observations and hypotheses which I bring to this field have not
been published in peer-reviewed journals and are not part of the
accepted understanding researchers and medical professionals have of
RLS/PLMD.
In September 2011, I sent a detailed 32 page account of my observations
and hypotheses to about 25 RLS researchers, including those who have
contributed most to this field in the last decade or so. As of
now, (August 2012), I haven't received any feedback on the
observations or hypotheses, but I am sure
I
will. Many of these researchers are medical doctors,
neurologists or have PhDs in neuroscience. I have no medical or
scientific qualifications and had only corresponded with one of these
people before. However, my experience in electronics
since 1968 (I am a 1955 model) helped me fault-find the disruption of
the
spinal cord's sensory and reflex circuits.
In May 2012, I received some encouraging
feedback from an Australian medical doctor who is a sleep specialist
and who sees many RLS patients: "Enjoyed your paper very much.
Welcome to the long haul of trying to improve the medical world, a
lifetime is needed. . . . You need to be patient and resilient in
this business, and success never guaranteed."
I also received a
message from a 24 year old UK man who found that both both ordinary and
decaf coffee, but not tea, when drunk late in the day or in the
evening, caused him to have RLS/PLMD:
#2012_06_08c.
In July 2012 I received an appreciative response from a US-based neurologist who read my material.
This disorder is unusual in many ways. It is a movement disorder
which is worsened by, or only occurs due to, periods of physical
inactivity such as sitting or lying down for an hour or more. It is not
a sleep disorder, but it invariably disrupts
sleep. It is the only disorder I know of in which either of these
two processes play a role:
Localized depletion of a precursor
chemical
(the amino acid tyrosine).
Low levels of random depolarization
(firing) of skin
sensory neurons, even when the skin in which their input terminals are
located is not being touched.
These two
situations have close parallels in electronics: power supply problems
and noise - meaning random fluctuations of electrons, such as those
which give
rise to hiss in an audio amplifier. So it was probably easier for
an electronic technician
such as me to identify these problems than for someone whose training
is in medicine or neuroscience.
I have been researching RLS/PLMD since 2004, when my wife Tina and I
were
married. Tina has had RLS/PLMD in her legs, arms
and torso since she was about 12. The symptoms were random,
occasional and
annoying, but got worse over time. Her doctors in Texas and
New York City listened to her reports but did not mention RLS.
Neither Tina nor I had heard of "Restless Legs Syndrome" before 2004,
when her symptoms became more serious. I found out about this
diagnostic category via a web search. In the USA in the late 2000s, RLS became widely
known - probably due to TV advertising of prescription drugs
which in recent years have been approved to treat the condition.
RLS is now better known in Australia too. The Internet has
facilitated much greater awareness of many previously little-known
health conditions.
Nowadays (2011 and beyond), for
a person with such symptoms as strong as Tina was suffering in 2004, I
think doctors would have no
hesitation in prescribing dopamine receptor agonist drugs - which are
routinely given to RLS/PLMD sufferers. These drugs have serious
potential side-effects, including compulsive behaviour, such as
pathological gambling, and augmentation - after a few years they make
symptoms
worse.
Another class of drugs used to combat RLS/PLMD are opioid
receptor agonists ("opioids") such as Methadone and Oxycodone.
These are indefinitely and are also frequently prescribed for
RLS/PLMD. However, opioids are addictive and potentially
debilitating,
commonly causing drowsiness, constipation and nausea.
Tina has never used any such prescription medications. I devised
non-drug techniques for reducing her symptoms. In recent years we
determined that the causes of
her worst symptoms were primarily coffee (including decaf) and
low iron levels. (In 2014 we found that potassium supplements
significantly reduced symptoms, but I am yet to update this page to
report on this fully.)
I believe that most people's RLS/PLMD problems result from low
iron,
interference from opioid receptor antagonists in coffee; and
interference
other drugs. (In 2011 I included caffeine as one of these drugs,
but in 2015 I am not convinced that it is directly involved in
RLS/PLMD, despite the generally accepted notion that it is.) I
propose that the common
susceptibility to these deficiencies and forms of interference is due
to a recently-evolved adaptation to the human
nervous system, which is triggered by soft touch to the arches of the
feet and which is not always deactivated when it
should be.
Tina may have some genetic proclivity to RLS/PLMD - I think quite a few
people do. Several research studies have identified genetic
variants which can affect the susceptibility to RLS/PLMD - though in
most cases it is not clear exactly which gene is involved; what the
gene normally does; or what it does differently in the variations which
worsen RLS/PLMD.
Some people may have suffered spinal injuries and infections - or their
nervous system may have developed (in-utero and shortly after birth) in
ways which make the symptoms more likely. Pregnancy and end-stage
renal disease are also well-known for contributing to the risk of
RLS/PLMD.
With good nutrition - including working with her doctor to ensure
her
iron levels are good - Tina now typically has most nights free of
RLS/PLMD
symptoms. She does not drink coffee (including decaf) or anything
else which contains caffeine - apart from chocolate, which contains a
little caffeine. We like chocolate but we find that more than
small amounts of dark chocolate or cocoa in the evening or perhaps late
afternoon is likely to cause RLS/PLMD
symptoms. Having some in the early afternoon and then going for a
4km walk does not seem to contribute to the risk of symptoms that
evening. Consuming excessive salt is another risk factor we have not
entirely eliminated.
Around 2009, I started getting occasional mild RLS/PLMD symptoms
too. This is mainly a curiosity to me - to experience what I have
been researching. My iron levels are OK. I stopped drinking
coffee and all other caffeinated drinks in 2004.
Now, if either Tina or I get any more than minor RLS/PLMD symptoms it
is usually
because we ate too much chocolate or cocoa, had too much salt, and/or
have not eaten enough protein in recent hours. Tina remains more
susceptible than I do, and her susceptibility is affected by her
menstrual cycle.
In November 2011, we only get RLS/PLMD symptoms going to bed if we have
overdone salt or chocolate. Tina often gets symptoms a few hours
before we wake up - such as on about 50% of mornings. For me,
this happens every week or two. I attribute this to a combination
of innate
proclivity to this condition - presumably genetic for Tina and
age-related for me, since I am 56 - the influence of salt and/or
chocolate and generally low levels of amino acids (including tyrosine)
in the bloodstream, since it is 12 hours or more since our generally
moderate- or high-protein evening meal. These symptoms are mild,
but disrupt the sleep of one or both of us. They are typically
one foot doing a set of ankle dorsiflexions every 40 seconds or so, as
depicted in the videos of Tina's foot below. We can make these go
away for a few hours - long enough to complete our night's sleep, by
using either percussive massage of the mid-lower spinal region and/or
taking two 500mg tyrosine capsules. Either approach seems to work
reliably - our symptoms are not so strong as to require both.
One RLS-suffering friend of ours, in her 50s, who drank one plunger
coffee and a few
instants a day reports that her symptoms (1/3 nights, while
sitting still and while in bed) have greatly diminished now she only
drinks one or perhaps two espresso coffees a week (when out
for the evening). She now drinks more tea, which generally has
less caffeine than coffee, and which is not known to contain opioid
receptor antagonists.
This friend and another in her 60s, who doesn't drink significant
quantities of coffee, both find that percussive massage of their
mid-lower spine area prevents or reduces their RLS/PLMD symptoms.
Both our friends pummel either side of their mid-lower spine with their
own fists.
The benefits are apparent within a minute or so and last for hours or
for the rest of the evening.
Our first friend mentioned above is experimenting with tyrosine
tablets, but now that she
drinks significantly less coffee than in the past, she has not had
enough RLS/PLMD symptoms to try the tyrosine with.
Other sufferers have independently discovered the
benefits of tyrosine and percussive
massage of the lower spinal region. Additionally they have also
discovered exercises which help them, such as inverting the body by
standing on the shoulders and elbows - perhaps with upside-down
bicycling motions of the legs. These
exercises are likely to cause physical movement and diffusion of
cerebro-spinal fluid in the lower part of the spinal cord, which I
believe is the main beneficial effect of percussive massage. When
I told our second RLS/PLMD suffering friend about this extreme form of
pre-bedtime
bicycling exercise that some people had discovered, she nodded
quietly, saying yes, she had done this too.
[#forums]
Feedback and discussion forums
If you are suffering from RLS or are
caring for
someone who is, and are interested in comparing notes, please email me (
../contact/).
There's an Australian RLS forum which I have not yet written to.
It seems to support of detailed messages, and in the first 4 weeks of
Nov 2011 had about 20 messages:
I wrote to this forum, but there is little activity: 12 or so messages in the first 4 weeks of Nov 2011:
The
Non-Pharmaceutical
Therapies
section of the
Restless Legs
Foundation RLS.org forum:
The RLS Support forum has searchable archives of 53708+ messages.
There were some discussions about my observations, hypotheses and
suggested techniques in this forum in November 2011, but the Moderator
does not want messages longer than a few paragraphs. Health is
complex and important, so this forum is not a good place to be
discussing my new observations and hypotheses. There were 230
messages in the first 4 weeks of Nov 2011, so it is a
lively forum.
I wrote to the WeMove.org RLS forum too, but it has little activity in general.
There were about 10 messages in the first 4 weeks of Nov 2011.
The
Movement
Disorder Society's
RLS Forum:
http://www.wemove.org/forum/.../Restless_Legs_Syndrome
No registration is required to read these forums. Registration is
required to contribute. (
If
you want to mention a commercial website of any kind, including any
page here at aminotheory.com, please delete "http://" and any "www." so
the forum software does not make convert the text into a
hyperlink. WeMove.org's policies prohibit hyperlinks to
commercial sites from their site, including in forum messages.)
Please remember this website, and my hypotheses, are not well known and
involve considerable differences from the mainstream understanding of
RLS. That understanding involves little or no idea about the
etiology (underlying mechanisms), other than a frequent assumption that
the pathology is in
the brain. Please don't assume that anyone on these forums knows
about this site, or that they would agree with this material if they
read it. Also, my suggestion that "Restless Limbs Sensorimotor
Disorder" (RLSD) replace "RLS" and "PLMD/S" is likely to be
controversial.
Spinal injuries and infections
Some people suffer RLS/PLMD primarily
or solely because they have
a spinal injury,
including one which resulted from a surgical procedure. I suggest
that anyone who suddenly developed RLS/PLMD which continued
indefinitely should discuss with their doctor the possibility that they
suffered a spinal injury or infection
at that time. I understand that vitamin B12 deficiency can lead
to neurological damage - which includes potentially permanent damage to
the brain and/or the spinal cord.
What I write below
is directed mainly at people who do not have spinal cord damage.
While percussive massage near the spine, to shake up the fluid in the
spinal cord, might reduce or eliminate symptoms for people with spinal
injuries,
I suggest that the dangers of compounding the injury are so great that
they should not do this without their neurologist's approval.
Spinal and spinal cord damage resulting from injury or infection
might involve circulatory
problems, or damage directly to the lower spinal cord circuitry, which
sense the skin of the foot arch. In my hypotheses, RLS/PLMD
involves this circuitry becoming hypersensitive, and being triggered
continually, to produce the sensory symptoms of RLS and the motor
symptoms of PLMD (involuntary toe-lifting, foot withdrawal and leg
withdrawal movements). Spinal damage may also reduce the
effectiveness of the pathway of neurons in the spinal cord from the
brain or brain-stem to the lower spinal cord, which I propose exists to
inhibit this highly sensitive mode of operation.
People with spinal damage may still have very serious RLS/PLMD
symptoms, even
if they use every non-drug preventative measure and remedy described
below, and whatever other
such measures there are.
Genetic or developmental difficulties
Similarly, to people with spinal
injuries and infections some people may have a genetic or
developmental abnormality which makes them unusually prone to RLS/PLMD
symptoms
despite all the right nutrition, exercise, avoidance of disruptive
drugs etc. I don't know of any research suggesting that
developmental difficulties may contribute to or cause RLS/PLMD
symptomatology, but it would not be surprising if this occurred as a
result of a person's nervous system building itself incorrectly.
Perhaps some people have a
genetic variation which reduces the level of iron in their
neurons. Perhaps some people have a genetic problem with Tyrosine
Hydroxylase or with some of the regulatory mechanisms for this enzyme,
which catalyzes the first step in converting tyrosine into dopamine and
which requires an atom of iron to function.
Neurologists
working with RLS/PLMD patients who have any of these underlying
problems - spinal damage, genetic predisposition, or some kind of
developmental abnormality - are at a serious
disadvantage at present, because there is no conventionally accepted
etiology for RLS/PLMD. I hope this material - or better
still the
longer not-for-publication PDF document I sent to RLS researchers
- will be of interest to such doctors, neurologists and other
specialists.
In 2012 or 2013 I plan to revise that PDF document and make it publicly
available on this website. This will be primarily for medical
professionals and researchers - including people such as myself who
have no formal qualifications. So I am keen for people who are
up-to-speed with neuroscience and RLS/PLMD to read the current version
and provide constructive feedback.
Your own research and comparing notes with others
Its strange that RLS/PLMD has resisted
explanation for so long.
Perhaps the research has been less vigorous than for other disorders
because no-one has ever died from the condition. However, it is
so widespread and disrupts so much sleep that surely some sufferers
have fallen asleep or made mistakes while driving, leading to serious
injuries and deaths. Chronic sleep disruption is also widely recognised
as leading to other health problems.
RLS/PLMD symptoms depend on a number of nutritional and other everyday
factors which are amenable to change. Experiments can produce
results
within minutes or days - and no special equipment or chemicals are
required. Percussive massage of the lower spine
region, by hand or with a motorized massager, typically (in our
experience, the experience of our friends and according to occasional
reports by other people on RLS websites, forums etc.) reduces or
eliminates symptoms in the legs in less than a minute, but not
affect symptoms in the arms. Percussive massage of the upper
spinal region can reduce or eliminate symptoms in the arms,
without affecting symptoms in the legs. (We have only observed
this arm-leg specificity ourselves. We can't reproduce this now since Tina no longer
has symptoms in her arms, and I have never had symptoms in my arms.) These
observations
provide strong support for the hypothesis that the pathology is in the
spinal cord.
Below (
#ownresearch) I encourage
people with sufficient time and interest to research their own, or
their spouse's, condition - with due care and caution about
safety. Doing so carefully and systematically, and
reporting the findings to other researchers, enables people to
contribute to the scientific process in ways which are more flexible
and hands-on than is possible with most formal research projects.
Such reports may also
motivate professional researchers - who have the required skills and access to funding and large numbers of
experimental subjects - to conduct larger trials.
Please don't try to become an amateur doctor or neurologist.
Doctors
and other specialists undergo a decade or so of intensive training so
they can make good judgments about safety and so they can reliably
apply a huge wealth of knowledge to medical problems.
They are continually striving to keep up with research in many aspects
of human health.
Doctors, medical specialists and nurses are usually not researchers. They generally don't base their clinical
decisions on hypotheses or observations which have not been widely
debated and accepted by other clinicians in their field. However,
this leaves them in
a tricky position with conditions like RLS/PLMD where no etiological
theory has been widely debated and accepted.
While your doctor can
advise you in general - particularly regarding safety - he or she can't
be making
house-calls at 3AM when the RLS/PLMD monster is ravaging you or your
loved-one. Nurses in hospitals spend all day or night caring for
patients, so they are perhaps in a better position to understand the
impact of this condition, and to experiment with ways of reducing its
occurrence. Assuming you are not being cared for by a nurse,
and your contact with you doctor and other specialists is at their
offices, during the day, you (and your spouse) are in the best position
to observe the problem
and experiment with methods of combating it,
provided you so so safely.
I can't tell you for sure what is safe or not. You need to decide
this yourself, ideally in consultation with your doctor or nurse.
RLS/PLMD will be somewhat different for different sufferers. With
care and
thought, it is possible to research it yourself - yielding information
which is more helpful specifically to you than anything you can read
about other people in
a book, website or journal article.
About us
I work with electronic musical
instruments, computer
programming and technical writing. Tina helps me with
electronics, looks after me really well, and works on her own
creative projects. Tina's blog with her friend Sandra involves
creative writing and photography:
Tina was born in Texas and I was
born in England. We live in Melbourne, Australia. Here we
are at a flower show in Ballarat, in April 2011:
My other websites are
http://www.firstpr.com.au
- Devil Fish electronic musical instruments, show-and-tell, many other
things - and
http://astroneu.com,
which concerns physics and astrophysics research projects, including
the mystery of the heating of the solar corona.
[#links]
Links
Here are some links:
- http://www.rls.org
The US-based Restless Legs Foundation. Clinical guidance is at: http://www.rls.org/Page.aspx?pid=524
in the form of a brochure and the RLS Medical Bulletin. (Below: #rlsorgpubs I link to both of these.)
A document on the name-change from "Restless Legs Syndrome" to
"Willis-Ekbom Disease" is: http://www.rls.org/Document.Doc?id=2128
- http://www.irlssg.org
The International Restless Legs Study Group. This page links to a document explaining their reasons for the name-change.
- http://www.rlshelp.org
The highly informative site of Mark J. Buchfuhrer M.D. in Southern
California. Includes a Word file to print and fill out to create
a personalized RLS Medical Alert Card. (See #word
below on reading it if your computer doesn't have Microsoft Word.) This
lists dozens of
RLS-worsening medications and potential alternatives which do not cause
such problems. A page rlsrx.htm
there has truly Comprehensive
Review of Medications used in Treating RLS and PLMD: 15,000+
words, regularly updated.
- Some RLS and Periodic Limb Movement Disorder videos from
YouTube. There are links to further videos of non-RLS conditions
in the self-diagnosis sub-sections 1 and 2 of the #help
section
below.
- 5P9L4tNukw0
PLMD
(Periodic Leg Movement Disorder) 2 (popcorn 0461)
An excellent example of a man's right foot moving in the characteristic
fashion while watching TV. Note the toe and foot being pulled up,
the repetition of this for second or two, and then 20 seconds or so of
calm before it happens again.
- k2eGoHk9AAc
Restless
Leg Syndrome? (BF109)
Intense RLS in the afternoon with foot rubbing in an attempt to sooth
it. I mention this below in the section on coffee and the history
of RLS.
- 2gyqT5pb5yU
Restless
legs syndrome (vintagelifelover) RLS squirming, blamed on
coffee, meat, processed food and Nilla
Wafers. As far as I know the meat, processed food and cookies
are not the problem, except perhaps for their salt content.
- UMJFZApu3vw
Ekbom's
Disease in Action (GBJonesIII)
12 minute video of a man sleeping, under sheets, but moving almost
continually due to what would probably be diagnosed as Periodic Limb
Movement
Disorder (PLMD).
[#summary]
Brief summary of my etiological hypotheses and some new observations
Please be sure to read the DISCLAIMER regarding health information at this site.
This section concerns scientific observations and hypotheses. It
is not intended as guidance
for anyone seeking to treat RLS/PLMD. (A more technically detailed and up-to-date summary is on a separate page: briefsumm/ .)
This brief summary lacks all the
references, further discussion and qualifications which a proper
account of any pathological condition should have.
For brevity,
the hypotheses are stated as if they were facts - but please remember
that these hypotheses
and new observations have not been
published in a peer-reviewed journal. Nor have they been
widely
discussed or accepted by mainstream RLS researchers.
My
not-for-publication 32 page PDF document (which I sent to about 25 RLS
researchers at the start of September 2011) contains more references,
discussion and qualifications.
Please don't
copy and paste this into blogs and other websites. Please link to this section of the
page: http://aminotheory.com/rlsd/#summary
. I will update this text and later replace it with a much
fuller body of material. So I don't want other copies of it
floating around on other websites.
The
terminology/ page explains some of the
terms used here.
Summary of new observations
[A] Percussive massage of the mid-lower back,
around the level of the navel, on either side of the spine (but not
touching the bony protrusions of spine itself)
reduces or
eliminates symptoms in the legs.
The effects begin within seconds or minutes and typically last for a
few hours.
This does not affect
any symptoms in the arms. Ordinary non-percussive massage - smoothly rubbing, kneading and pressing firmly - has no effect.
[B] Percussive massage
of the upper spinal region,
below the neck, between the shoulder blades (again, don't touch the
spine itself, or its bony protrusions, just the ribs and muscles on
either side)
reduces
or eliminates symptoms in the arms. The effects begin
within seconds or minutes and typically last for a few hours.
This does not affect
symptoms in the legs. Ordinary non-percussive massage - smoothly rubbing, kneading and pressing firmly - has no effect.
[C] If there are also symptoms
in the torso (usually the pattern is legs, arms and then torso, as
overall severity rises) these may be relieved to some extent at least
by
overall percussive massage of the whole area of the back , including
close to the spine, but again, not actually contacting the spine
itself. (For more details of these three types of massage, see
below:
#help14_comprehensive_massage.)
[D] Oral tyrosine,
such as 1, 2 or 3 x 500mg tablets or capsules (tyrosine, AKA L-tyrosine
- we haven't tried N-acetyl-tyrosine)
reduces or
eliminates symptoms in the legs, arms and torso.
Effects begin within five to ten minutes and typically last for two
hours or so, depending on dose and severity of the symptoms.
The above four observations are consistent with the hypothesis that
RLS/PLMD symptoms result (in the context of other precipitating factors
such as low iron and/or opioid receptor antagonism and/or dopamine
receptor antagonism) largely or entirely due to a localized depletion
of tyrosine in the nociceptive (pain sensing) reflex generating
circuitry in the spinal cord. It is also consistent with reports
by other people on RLS forums and the like that exercises which
stretch, exercise, vibrate or invert the lower spinal area are helpful
for reducing or preventing symptoms.
[E] While caffeine is generally
(over many hours and days) disruptive of sleep and may contribute
directly to RLS/PLMD symptoms and while acute doses of caffeine or at
least of caffeinated coffee
may for
some people
reduce symptoms and induce sleep for an hour or so (as some report,
this is not our experience), Tina and one of our RLS/PLMD-suffering
friends have discovered a link between coffee and RLS/PLMD symptoms
which does not seem to be related to its caffeine content. (Our
other RLS/PLMD-suffering friend hardly drinks coffee.) We
observe that
coffee
of any kind, including decaf (which has about 5% the ordinary caffeine
content) consistently worsens or causes RLS/PLMD symptoms. Some
other compounds in coffee appear to be responsible for the great
majority of what we previously thought were naturally occurring
symptoms
due to some fundamental disorder in the body.
This is consistent with the well researched, but little known, 1983
discovery that coffee of all kinds
contains significant quantities of mu opioid receptor antagonists.
Researchers have identified the major substances and shown that they
are created in the roasting process. (See another page on this site: ../coffee.)
[F] With regret, we must report
that we find sufficient quantities of
dark chocolate
or organic raw cacao powder (as mixed into a drink) precipitate
RLS/PLMD
symptoms. Presumably ordinary cocoa (which is made from roasted
cacao beans) does the same. This only appears to be the case if
we have the chocolate or cacao in the evening, or perhaps late
afternoon, regarding symptoms appearing when we go to bed, which is
typically after midnight. Having some in the early afternoon,
followed by a 4km walk, does not seem to cause much trouble.
The effect of raw cacao seems to indicate that whatever is causing this
is not due to the roasting process or whatever else goes into
chocolate. There is presumably some caffeine and a lot of
theobromine in these foods. The researchers who discovered mu
opioid receptor antagonists in coffee found no such activity in
chocolate or any other foods or drinks they tested. The mechanism
behind this is unknown, but it might involve dopaminergic antagonism,
some effect on blood flow, transport of amino acids, effects on
Tyrosine Hydroxylase or some as-yet undocumented opioidic
disturbance. (Perhaps raw cacao has a stronger effect in causing
or worsening RLS/PLMD than the same quantity of cocoa.)
[G] When symptoms are
present in the legs, applying a
very light touch,
(a gram or a fraction of a gram as force) such as with a pencil-tip or
matchstick,
to
the arch of the foot elicits an instant and powerful foot - and perhaps
leg - withdrawal action.
This
only occurs when the arch of the foot is touched in this way, not the
heel, ball or toes and not the top of the foot or anywhere else in the
leg. It does not occur when there are no RLS/PLMD
symptoms. Nor, when there are symptoms, does the reflex response
occur if this area is rubbed firmly, deeply and smoothly.
[H] Similarly, only when
symptoms are present in the arms, a
very light touch to
the centre of the palm of the hand (the softer skin, somewhat
equivalent to the softer skin of the arch of the foot) -
elicits an instant
and powerful hand and perhaps arm withdrawal action.
The hand lifts backwards, away from where the palm is, with the fingers
becoming outstretched (the opposite of gripping or pushing the palm
down) when a very light touch sensation occurs in the centre of the
palm of the hand. Similar light touch anywhere else on the hands
does not elicit this sharp hand withdrawal and perhaps arm withdrawal
response. Again, firm, deep, smooth rubbing does not elicit any
such response.
These withdrawal reactions are clearly spinal reflexes, but they are
not triggered by a noxious stimulus - just a very light touch which
would ordinarily be consciously perceptible, perhaps in a ticklish
way. [G] and [H] are entirely consistent with my hypothesis that
disorder underlying RLS/PLMD symptoms involves a special (I suggest
human-specific) reflex response which is ordinarily inhibited, but
which becomes extremely sensitive when symptoms are present, due to
inadequate activation of dopamine receptors and/or opioid receptors, in
the spinal nociceptive/reflex circuits concerning the foot arch.
Similar circuits evidently exist for the hands and the torso, but these
are either less sensitive to start with, and/or are less susceptible to disruption, so symptoms typically occur first
and worst in the feet/legs, then in the hands/arms and finally in the
torso.
[I] Applying a local anesthetic
such as EMLA (prilocaine and lidocaine
http://www.emla.co.uk)
to the arches of both feet reduces or eliminates symptoms in the feet
and legs. (We haven't tried this with the hands, since Tina no
longer has symptoms there.)
[G], [H] and [I] are consistent with my hypotheses regarding the
pathological disinhibition of a foot arch protective reflex triggered
by
non-noxious soft touch, with the RLS/PLMD symptoms being generated even
in the absence of any such touch by what I argue is the low but
normally constant, level of random depolarizations of cutaneous
mechanoreceptor neurons in the foot arch. These observations are
consistent with the hypothesis that partially anesthetizing these
neuron's sensory terminals reduces this low level of random
depolarizations to the point where symptoms are reduced or eliminated,
despite the spinal nociceptive/reflex circuitry being pathologically
hypersensitive to input from these neurons.
We haven't tried anesthetizing the hands, or just one foot. A
prediction of these hypotheses is that anesthetizing just the palms of
the hands would diminish or eliminate symptoms in the arms, but not the
legs, and likewise anesthetizing the foot arches would reduce or
eliminate symptoms in the legs, without affecting any symptoms which
may be in the arms. A further prediction is that if the symptoms
were in both legs, anesthetizing just one foot arch should reduce or
eliminate symptoms largely or entirely in that leg alone.
Likewise for anesthetizing a single palm when there are symptoms in
both
arms.
We find the following mixture better than EMLA in that its benefits
seem to last for hours or perhaps the rest of the night in the case of
milder symptoms: 40% Clove Bud Oil, 40% food-grade cold-pressed
coconut oil and 30% isopropyl alcohol. We have found this very
effective when applied to the whole foot: heel, arch, ball and
toes.
I am not convinced that this idea of anesthetizing the foot arches will
be acceptably safe on a regular basis, so it is not one of the
suggestions I make below. It does involve drugs, albeit applied
to the
skin. But they go into general circulation through the skin and I
cannot advise on the long-term side effects of this. Nonetheless,
this is a powerful and instructive research technique - and I
think the results we have observed will be easily replicated and
provide strong support for my hypotheses.
[J] We have also observed what
I regard as "crosstalk" within the spinal nociceptive/reflex circuits
where
cool
skin on the lower back, upper back, shoulders or even the arms will
precipitate periodic foot movements.
This appears to be consistent with my hypotheses in the context of the
research into in-utero and/or post-natal developmental pruning of
sensory input to these circuits, and how it may be imperfect, along
the lines suggested by Chapter 12 of "The Science of Pain" (
Appropriate/Inappropriate Developed
Pain Paths by Jens Schouenborg
website
see
#help10 and
#ownresearch
below).
Summary of my new etiological hypotheses
For brevity,
the hypotheses are stated as if they were facts - but please remember
that these hypotheses
and new observations have not been
published in a peer-reviewed journal.
[1] Humans have a
recently evolved (~3 million years or so)
soft-touch foot arch reflex
response which lifts the
toes and the foot, in response to a light touch sensation in the soft
skin
of the foot arches - not the heel, the ball of the foot, or the toes.
This
response is ordinarily enabled when walking on potentially spiky
ground, or in swamps, to avoid puncturing the soft skin of the foot
arch. Humans are the only surviving species to have foot arches.
The foot arch is a necessary
consequence of a flexible foot which concentrates most weight on the
heel and the distant ball and toes, in order to gain the greatest
purchase on the ground, to facilitate the forwards-backwards balance
which
is so important for a bipedal species. With only two feet for
locomotion, our bi-pedal ancestors could not afford to have even one
foot punctured and infected, so there would have been strong selection
pressure to develop protection for the arches of the foot.
[2] This reflex
response is extremely sensitive, and is normally
turned off by a population of so-far unidentified dopamine-producing
(dopaminergic) neuron output terminals in the spinal cord. These
would be close to some dopamine receptors which inhibit the
interneurons which
give rise to the reflex response. The brain or brainstem
evidently activates these descending dopaminergic neurons most of the
time, including when we are sitting still or sleeping, to prevent false
triggering of the foot withdrawal reflex response. Whatever part
of the brain or brainstem (I assume) turns on this descending
dopaminergic pathway evidently turns it off when we are walking on
dangerous ground.
[3] This is a
modification of the standard foot withdrawal reflex
which is common to mammals in general and to primates and apes in
particular. The genetic instructions which create this recently
evolved soft-touch
sensitive system and its descending dopaminergic inhibitory system also
creates, as a probably non-functional side effect, similar arrangements
for the hands, the torso and perhaps the face. (To do - find the paper
which reports RLS-like symptoms and movements in the face.) This
system in the
hands would help prevent the palm of the hand being punctured if we
grip a spiny tree-branch, so it may be adaptive for the same pattern to
be repeated in the hands.
[4] RLS sensory symptoms and
PLM (Periodic Limb Movement) movement symptoms result primarily from
some combination of the following three processes. These may be caused or
aggravated by spinal injuries or infections and/or by genetic or
developmental problems.
(4a) - Inadequate dopaminergic
inhibition of these foot-withdrawal reflex circuits in the spinal
cord. This is likely to be due to lack of iron in the
dopaminergic output terminals, and/or lack of tyrosine near these
output
terminals, and/or due to partial blockade of the dopamine receptors,
due
to dopamine receptor antagonists, such as the drug Phenergan
(promethazine).
Please see point [5] below for a more detailed explanation of localized
depletion of tyrosine resulting from long (typically hours) periods of
physical inactivity (sitting or lying down, rather than walking,
running, stretching or exerting a lot of physical effort).
(4b) - These and other nociceptive (pain sensing) circuits in the
spinal
cord being more than usually sensitive due to inadequate activation of
their opioid receptors, such as due to ingestion of opioid antagonists
in coffee, or the use of drugs such as naloxone.
(4c) - A sufficiently high level of "noise-driven" - random - firing of
the soft-touch foot-arch sensory neurons, in the absence of any of the
point-contact very light touch sensations which normally stimulate
them. This is "noise" in the electrical engineering sense - random
events caused by thermal motion of electrons. The same process in
an audio amplifier creates audible "hiss". This low level random
firing is probably normal and would not result in a conscious
perception of touch, or in the foot withdrawal reflex. However,
if the reflex
system was being properly inhibited by the descending dopaminergic
pathway and by sufficient activation of opioid receptors, this random
low level of sensory neuron depolarization can be sufficient to trigger
RLS sensations and PLM reflex movements.
[5] RLS and PLMD are diagnostic
categories which arise from a common disorder which I suggest be called
Restless Limbs Sensorimotor Disorder (RLSD). This is a
movement disorder which occurs after (or is
worsened by) periods of stillness -
lack
of movement. This has perplexed
researchers for decades. The most likely explanation for this is
that the constant need for tyrosine in a narrow (say 1mm diameter, a
few cm
high) column of the dorsal
horn of the lower spinal cord, in order to produce the constant supply
of dopamine to inhibit the newly evolved highly-sensitive,
foot arch soft-touch-driven foot withdrawal reflex response, leads to a
localized
depletion of tyrosine in
this narrow column. I propose that during active movement such as
walking, running, etc., the cerebro-spinal fluid (CSF) in the spinal
cord is constantly agitated, causing it to diffuse several mm over a
period of seconds or minutes. So even if the capillaries in this
~1mm diameter (my guess) column can't supply tyrosine from the blood to
the CSF at the required rate, the
dopaminergic output terminals in this column will receive fresh
tyrosine-rich CSF from nearby parts of the spinal cord, via ordinary
physical activity driving movement and diffusion of the CSF. When
we sit still, or lie down, for long periods, this diffusion is reduced,
and it seems that - at least for RLS/PLMD sufferers - the dopaminergic
output terminals deplete the CSF in
their column of tyrosine, to the point of being unable to produce
enough
dopamine to inhibit the touch-sensitive foot-arch reflex response.
[6]
From the above, it follows that we can reduce or eliminate RLS/PLMD
symptoms
by one or more of the following:
(6a) - Increasing the activation of the dopaminergic receptors in
these spinal circuits. The best way would be by ensuring there is
sufficient iron and tyrosine in these parts of the spinal cord.
(See above regarding percussive massage, and the section below
regarding non-drug measures to combat RLS/PLMD.) Dopamine agonist drugs
(compounds which activate dopamine receptors) will work too, but these
affect the entire
nervous system, including many parts of the brain, and can lead to augmentation and side-effects including
compulsive behavior (punding
1999-paper) and
pathological gambling.
(6b) - Reducing the level of opioid receptor antagonists, such as by
reducing or eliminating the use of any kind of coffee. (Similarly
reducing or eliminating caffeine or any other drugs which disrupt sleep
or in some other way contributes to RLS/PLMD.)
(6c) - Increasing the levels of opioid receptor agonists, such as by
increasing endorphins (such as through exercise or perhaps as one of
the consequences of percussive massage of many parts of the body) or by
taking opioid
drugs such as methadone (which are potentially addictive and have
serious
ill-effects).
(6d) - Reducing the level of "noise" firings of the sensory neurons
which can activate this foot-arch protective reflex system, to a lower
level than normal, even if this means these sensors are not able to
properly sense the lightest touch. See observation [I]
above regarding anesthetizing the skin of the foot arch.
[#help]
Help for sufferers - non-drug techniques for combating RLS/PLMD
Before considering this material, be
sure to read and accept the
DISCLAIMER.
Apart from the advice on iron, which is entirely conventional and
accepted by all RLS/PLMD doctors and researchers - and probably the
material on Folate and Magnesium - everything in this section
is novel and not supported by research published in peer-reviewed
journals. The research I cite on opioid receptor
antagonists in
coffee is the work of conventional researchers and is published in
peer-reviewed journals. (
../coffee/)
This research seems to have flown under
the radar of pain and RLS/PLMD researchers. However, its easy to
see
that opioid receptor antagonists are likely to cause or worsen RLS/PLMD
and
pain disorders such as fibromyalgia.
This is free information from an electronic technician with no medical
qualifications. Please let me know of your experiences -
positive, negative or neutral (
../contact/).
[#rlsorgpubs]
Please consider these suggestions in the
context of the conventional view of Restless Legs Syndrome and check
your own symptoms against the conventional Diagnostic Criteria.
The best documents for these are from the Restless Legs Syndrome
Foundation website's publications section (
http://www.rls.org/Page.aspx?pid=524):
You don't need to understand or accept the hypotheses in the above
#summary section in
order to
consider accepting the following suggestions. You do need to
ensure that whatever you do or stop doing is safe. I can't tell
you for sure what is safe for you. Your doctor is the best source
of advice on the safety and appropriateness of various treatment
options.
The subsections below are:
- 01 - Self-diagnosis, with videos
- 02 - Other patterns of movements which are
not RLS/PLMD
- 03 - Ensure your iron levels are good
- 04 - Do not drink coffee of any kind,
including decaf
- 05 - Reduce or ideally eliminate your
consumption of caffeine
- 06 - Dark chocolate and cocoa seems to
worsen or cause RLS/PLMD
- 07 - Excessive salt seems to worsen or
cause RLS/PLMD
- 08 - General nutrition, including Magnesium
and Calcium
- 09 - Avoiding drugs which worsen the
condition
- 10 - Sleeping position and keeping warm
- 11 - Unusually high or low levels of
exercise
- 12 - Protein meals and snacks
- 13 - Tyrosine capsules or tablets
- 14 - Percussive massage
- 15 - Other factors and techniques
help01 - Self-diagnosis, with videos
Please
be sure to read the Diagnostic Criteria on pages 2, 3 and 4 of the
RLS.org RLS Medical Bulletin linked to above #rlsorgpubs.
Here are
some further notes:
If your symptoms are "restlessness" (hard to describe feelings of
creepy-crawlies, twitchiness etc.) in the legs, arms or torso AND these
symptoms typically only arise, or get much worse, following periods of
physical inactivity, then you would probably meet the
RLS
diagnostic criteria. "Periods of inactivity" means sitting
still
or lying down, with little or no movement or exertion, for periods such
as an hour or more. Some sufferers may develop the symptoms with
shorter periods of inactivity.
Some sufferers report their sensations as painful, but I recall a
research paper which indicates that they meant a low-order pain, rather
than something acute.
Tina never describes her RLS sensations as painful. By contrast, I
have
sometimes felt the whole soles of both my feet, including the toes, to
be
sore. In these instances, it has been my impression that reducing
or stopping the underlying
RLS/PLMD mechanism with percussive massage near the mid-lower spine,
and/or taking 2 x 500mg tyrosine tablets with half a glass of water,
reduced the RLS urge to rub my feet
together and reduced the soreness. This would be consistent with
what I understand about the operation of the spinal cord's nociceptive
(pain-sensing) circuits - they can become more sensitive when another
nearby pain-sensing system is moderately activated.
An intense case of RLS foot-rubbing interrupted by involuntary
movements can be seen in the video
Restless
Leg Syndrome? (BF109) in the Links section above.
If your feet or legs - or hands, arms or torso muscles
- make involuntary movements AND this is associated with periods of
physical inactivity AND if the movements were numerous enough per hour
AND occurred with suitable timing (such as 20 to 40 seconds or so
apart), you would probably meet the
PLMD
diagnostic
criteria. These movements can happen
when
awake or asleep.
The underlying mechanism which gives rise to both the RLS and PLMD sets
of diagnostic criteria is is a movement disorder, which disrupts
sleep.
The mechanisms are the same when asleep or awake. My hypotheses
(summarized above)
locate all the problems in the spinal cord. I know of no evidence
that there's anything wrong with sufferer's brains, legs or arms.
Please
read
these hypotheses so you can at least partially understand my viewpoint
on this disorder,
and how it differs from the viewpoint of many conventional researchers,
who tend to assume it
is a brain disorder and whose treatment options (after sorting out iron
levels and perhaps magnesium) are largely based on prescription drugs
with serious side effects.
Here are two 15 second videos of Tina's right foot doing a
single typical Periodic Limb Movement while she is asleep.
These are not streaming videos like
from YouTube servers. Your browser
will download the whole file - which may take a minute or two - and
will pass it to an MPEG viewer program in your computer. Each
file is 5 Megabytes and plays for 15 seconds. I suggest
right-clicking the link or image and opening the video file in a
separate browser window.
 Tina-RLSD-2008-10-23.mpeg
Tina-RLSD-2008-10-23.mpeg
This pink sock video above and the barefoot one below depict typical
RLS/PLMD foot movements while Tina is sleeping.
 Tina-RLSD-2006-08-25.mpeg
Tina-RLSD-2006-08-25.mpeg
These occur with intervals
typically in the 20 to 40 second range. My
right foot occasionally does much the same thing, when I am awake - but
usually only due
to excessive chocolate, salt or perhaps inadequate protein in recent
hours.
 Tina-RLSD-2006-10-12.mpeg
Tina-RLSD-2006-10-12.mpeg
This one shows a common foot
stretching response, which may be semi-voluntary, since Tina is
being partially awoken by the sensory disturbance and is, by habit,
stretching or
rubbing her feet to try to reduce the problem.
If Tina pulls her feet towards herself, so the soles of her feet are
pressed against the bed and her knees are elevated, this is a good sign
that the RLS/PLMD monster is at work; likewise foot rubbing or
shaking. Tina's feet can also do a gentle but quite rapid (~3
cycles a second, like a pure sine-wave) ankle twisting motion
where the toes are not pulled upwards. Neither she nor I can do
this
consciously ourselves except in a coarse and jerky manner.
help02 - Other patterns of movements which are
not RLS/PLMD
If you have
muscle spasms in the legs
arms and torso, while falling asleep (you may not notice this, but your
bed-partner will) and you
recently consumed a lot of caffeine - say a cup of coffee, or an
"energy drink" earlier in the evening or that day, then I suggest that
this is
probably not related to RLS/PLMD. I think it is more likely a
direct
result of the
caffeine.
These spasms are random, rough and sudden, perhaps with the hand being
drawn in
and the foot going down. Many muscles fire suddenly within a
second or less, in ways which
would not be possible to elicit by conscious commands from the
brain. RLS/PLMD movements are
characteristically of the toes and foot moving upwards, and the fingers
pulling back, with the hand and arm pulling away from what the palm
might be touching. The RLS/PLMD movements tend to repeat every 20
to 40 seconds. The caffeine-caused spasms are more erratic and
random - and it is my impression they only occur at the threshold of
falling asleep.
One common night-time movement pattern which has nothing to do with
RLS/PLMD is the
Hypnic Jerk:
http://en.wikipedia.org/wiki/Hypnic_jerk
also known as
Hypnagogic Jerk. This occurs when falling asleep,
without warning. It
involves a sudden, surprising, sensation of
falling for a split second. It is my impression that these do not
usually repeat
themselves more than once a night. I guess I have one or two a
year.
A serious and fortunately rare movement disorder which may affect the
legs is
RSD/CPRS
- which is apparently usually a result of injury. The leg spasms
depicted in
this YouTube video
qE_OwuilOew
do not resemble those of RLS/PLMD since they involve lots of
muscles being activated erratically at once.
There is a separately recognized leg movement disorder
called "
Nocturnal Quiescegenic Dyskinesia":
http://www.kicking-legs.com
. The movements in this YouTube video:
QOiRmXh4CA4 are
quite unlike RLS/PLMD. The movements in this video are
centered in the thighs and hips, with none of the pulling back of the
toes, or
foot withdrawal motions which are characteristic of RLS/PLMD.
In June 2012 I had an interesting discussion with one of our electronic musical instrument clients about
foot tapping.
He is a 37 year-old musician and computer programmer who is bristling
with creative energy and enthusiasm.
With his foot on the floor while sitting in a chair, his toes push
downwards, lifting the ankle, calf and knee, several
times a second in a resonant bouncy fashion. This pattern may
continue for seconds to tens of minutes. Since he was a child
he has frequently tapped his foot. This is when he is sitting in
a chair - never while lying in bed - so his foot must be on the
ground or a footrest. It tends to happen when he is more tired, and not so much
in the morning or after sleep. It happens more when he is
concentrating on technical matters such as computer programming, but
not so much when painting or making music. He is observant and is
interested in health, so he has noticed and thought about this
tendency for many years. He does not consider it a
disorder or a disability. It is, nonetheless, a pattern of
movement which might be considered "Restless Legs".
He finds many factors make it occur more strongly, including especially
sugar. He used to drink large quantities of fruit juice; but now
has minimal intake. He speaks highly of Australian author David
Gillespie's
Sweet Poison - the Quit Plan http://sweetpoison.com.au
. He reports that these factors seem to increase his foot
tapping: coffee (both ordinary and decaf); tea (caffeinated, not
herbal); Coca Cola, including sugarless, caffeinated Coke Zero;
tobacco; bad posture when sitting in a chair, such as leaning forward;
placing weight on the leg; intense thoughts. Typically he taps
with his left foot, without really thinking about it, but his right one
can do it too. I think it tends to be one or the other, not
both. He can stop the movements if he thinks about it, which is
totally
different from the movements of PLMD. Opioid drugs reduce it, I
guess due to opioid receptor activation causing drowsiness, and
generally relaxing muscles. This may explain why decaf coffee -
with ~5% the
ordinary amount of caffeine, but with coffee's usual amount of mu
opioid receptor antagonists - makes it worse. These antagonists
would reduce the ordinary level of activation due to the body's own mu
opiate receptor agonists, as mentioned in the section below on coffee.
This pattern of foot tapping is common - I do it myself at
times. It seems unrelated to the movements of RLS/PLMD because it
does not occur when lying down in bed, because it is continual and
rhythmic, because it can be consciously inhibited and because
(according to this fellow) he can easily and happily synchronize it
with music, especially around 140 beats-per-minute. There are
foot-tapping movement disorders, but I am not convinced that what this
fellow reports is one of them.
help03 - Ensure your iron levels are good
Many people are at risk of low iron
levels, particularly menstruating women and people (such as me) who
don't
eat meat. There are various oral iron supplements, but you should
work with your doctor on this.
Your doctor can organize a blood test to assess the levels of iron in
your blood, and perhaps most importantly the levels of iron stored in
your blood in ferritin. He or she can advise you on the need for
supplementation and on the best type to use. Your doctor will
also test whether you have any iron regulation problems.
The body has other storage mechanisms for iron, but ferritin in the
blood is the one
which is most easily measured. There is a little iron in solution
in the blood plasma, but this is kept to a safe level, since iron ions
(iron atoms missing some electrons) in solution are highly reactive and
destructive.
A ferritin molecule is a cage for
containing iron atoms bound to other atoms in a way which protects the
rest of the body from these highly reactive and potentially destructive
atoms. Details:
http://www.chemistry.wustl.edu/~edudev/LabTutorials/Ferritin/Ferritin.html
Compared to the digital nature of DNA, and the subtle chain-based
folding of protein, ferritin strikes me as being like a robust
piece of Victorian-era mechanical engineering!
Iron is needed for many functions in the body. Its importance for
RLS/PLMD is that the complex enzyme Tyrosine Hydroxylase (TH) requires
an atom of
iron in order for its catalytic site to function. TH catalyzes
the conversion of the amino acid Tyrosine into
L-DOPA in the output terminal of dopaminergic (dopamine-producing)
neurons. The L-DOPA
is converted into dopamine by a second enzyme which never gives any
trouble. Inadequate iron levels will reduce
the efficiency of TH, so leading to the reduced dopamine production
which is well recognized as a causative factor in RLS/PLMD.
While iron deficiency is a common cause of ill-health, iron poisoning
of children who take iron supplements is a leading cause of
death. Please heed the advice in this University of Maryland
Medical Center article:
Iron
poisoning is the most common
accidental poisoning in children. Keep iron supplements in childproof
bottles and out of the reach of children.
help04 - Do not drink coffee of any kind,
including decaf *
There are many health reasons for
avoiding caffeine, including the fact that it disrupts sleep, and
causes
tiredness, irritability and anxiety. I also think it stunts
creativity, reduces our ability to relax, and drives people to use
other harmful drugs, such as alcohol and tobacco, in an effort to calm
their anxiety.
It is commonly stated, assumed and understood that caffeine, or
excessive caffeine (whatever that might be) contributes to or causes
Restless Legs Syndrome. I don't recall reading any research which
supports this assumption, and I have read a lot of RLS research!
Since one of the major impacts of RLS/PLMD is to disrupt sleep, and
since caffeine (and alcohol) are commonly used drugs which disrupt
sleep, it makes sense to cut down on these or eliminate them, in
general, especially if RLS/PLMD is disrupting sleep.
However, if you feel you must use caffeine, I suggest you drink tea
instead. (Caffeinated soda drinks and high-caffeine "energy drinks"
contain more caffeine and are much less friendly to teeth.)
Coffee contains opioid receptor
antagonists. These opioid
receptor antagonists are unrelated to caffeine - decaf coffee
contains about 5% of the usual amount of caffeine, but the same levels
of opioid receptor antagonists. Please see a separate section of
this website concerning this, with links to the peer reviewed journal
research papers:
* However, please see the above page which has a note near the start of
the likely protective effects of coffee, decaf or not, against both
Parkinson's disease and Alzheimer's disease.
These were discovered in 1983 and more recent research has identified
the major mu opioid receptor antagonists, which are not present in raw
coffee beans but which are created by the breakup of some of the
molecules during the roasting process.
These compounds, such as
4-Caffeoyl-1,
5-quinide:
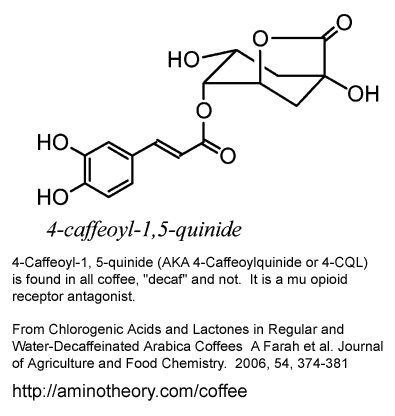
are unrelated to caffeine and have a high affinity for opioid
receptors. They occupy opioid receptors but do not active
them. This reduces the number of receptors which are open to
being activated by the natural levels of endogenous (produced in our
bodies) opioid receptor agonists, such as endorphins and
enkephalins. These are known collectively as "endogenous
opioids".
Normally, the activation of opioid receptors in the spinal cord by
these endogenous opioids reduces our sensitivity to pain, and to the
reflex reactions which the spinal cord generates to move limbs away
from noxious stimuli. (The same spinal cord circuits produce both the
pain signals to the brain and the muscle activation signals to withdraw
limbs from noxious stimuli.) Opioid receptor antagonists block
these receptors and so make the spinal circuits more sensitive to pain
and to creating reflex limb withdrawal motions . I propose that
when RLS/PLMD sufferers are having symptoms, these circuits are become
hypersensitive in RLS/PLMD - so any antagonism of these receptors will
make symptoms worse.
Tina and one of our
RLS/PLMD-suffering friends have found that reducing or eliminating
coffee of all kinds significantly reduces the incidence of
RLS/PLMD.
In June 2012 I received a message from a 24
year-old man from the UK who found that both ordinary and decaf coffee
seemed to cause RLS/PLMD. He wrote:
I've
suffered (albeit lightly) with RLS during and shortly before sleep
after drinking coffee. It's a bad habit of mine and I decided to move
onto decaf to solve the problem of my RLS during sleep.
I soon discovered this
wasn't the case. I can directly link drinking decaf coffee and RLS
during sleep as I've tested it upon many occasions. Drinking no decaf coffee in the evenings I experienced no RLS for several nights in a row.
Drinking decaf in the evenings even a few hours before sleep I suffer RLS.
The brand of coffee was Nescafe, though I've experienced it with other brands. I'm a 24 year old male, if that helps.
I'm no scientist, nor a doctor. I just wanted to do some quick Googling and found your page AminoTheory.com.
I hope my experiences help or at least add another number to the statistics.
I hope to find more details of his observations, such as his symptoms
and what other caffeinated drinks, including coffee, he may be drinking
earlier in the day.
I suspect that these opioid receptor antagonists in coffee are also
highly likely to disrupt sleep and cause, or worsen, pain disorders
such as
fibromyalgia.
I would not be surprised if a great deal, perhaps the majority, of
the
total symptomatology of RLS/PLMD is caused by these opioid receptor
antagonists in coffee. (Though some of the most severe sufferers
who have spinal injuries, nutritional disorders or strong genetic
predisposition will no-doubt suffer bad symptoms without any coffee or
caffeine consumption.)
Vintagelifelover on YouTube has
a 2 minute video
http://www.youtube.com/watch?v=2gyqT5pb5yU
of her squirming legs.
"You gotta keep stretching, moving . .
. and stretching, your legs . . . Driving you nuts, because something
inside makes them want to go. I fell off the raw food truck . . .
I started to drink coffee,
eat
meat and processed food. What happens? You feel
terrible! There were cookies this morning, yes there were -
Nilla Wafers (link)- and now I can't stop with my silly legs!"
She blames the unhealthy food - but I think it was the coffee. Tina and I occasionally have
Nilla Wafers sent by a friend from the USA, and there's no sign that they contribute to RLS/PLMD.
Many people drink coffee every day and think it helps them,
overall. I used to think this about tea and coffee.
A few people finding that coffee of any kind makes RLS/PLMS much worse
does not establish beyond reasonable doubt that this is the case for
all other
people. But it does point to something which is easy to try, and
may provide significant benefits for many people.
Anyone reading the above will be able to consider that perhaps
coffee, for whatever reasons, is causing them long-term difficulties
which they may not have realized, thinking that RLS and other problems,
such as tiredness, anxiety etc. are just part of life, or part of
getting older.
Caffeine generally perks us up, which would be great if that was all
that happens. But after a few hours the positive effects wear off
and we are left more tired for a day or two than if we had not used
it. This might be a good deal if we achieve something great in
the few hours and don't have to worry about the impact of the
tiredness, anxiety etc. To call caffeine a "stimulant" is to
describe only its short-term effects.
Please see a section below for more
details regarding coffee and RLS/PLMD, including the history of coffee
and how the RLS sufferers Thomas Willis observed in 1672
may have been coffee drinkers: #coffee.
In March 2015, I mentioned these opioid antagonists and RLS/PLMD in a letter:
See an update to this regarding caffeine and restless legs syndrome:
../briefsumm/#ccc .
help05 - Reduce or ideally eliminate your
consumption of caffeine
Caffeine, as found in tea, coffee,
soft-drinks / soda-pop and high-caffeine "energy drinks" is an
addictive drug which, amongst other things,
disrupts sleep.
RLS/PLMD disrupts sleep, and I think caffeine probably contributes to
the
RLS/PLMD processes, though I am not sure how.
More information below in the
#coffee
section. Please remember that decaf coffee contains, very
approximately 5% of the caffeine of ordinary coffee, which I think is
quite enough to keep people addicted and to disrupt sleep. But if
you feel you must use caffeine, I suggest you avoid coffee of any kind for the
reasons noted above.
Perhaps if the caffeine or coffee is drunk just before vigorous
exercise, such as a long, fast walk or a bike ride, the ill-effects my
be diminished significantly due to the compounds being metabolized and
excreted quickly, rather then remaining in the nervous system at high
concentrations for many hours or a day or so. Short-term use of
caffeine after not using any for a
few days can certainly boost physical endurance and perhaps mental
performance for a few hours.
However, I
think that using it continually - as most people do - does not improve
mental or physical performance. One of the ways caffeine
interferes with neurons is as an adenosine receptor antagonist.
If humans had better overall performance with less activation of
adenosine receptors, evolution would have quickly lead to most or all
of us having less sensitive adenosine receptors.
help06 - Dark chocolate and cocoa seems to
worsen or cause RLS/PLMD
This heading should be preceded by "
UNFORTUNATELY
. . . ".
Lacking X-ray vision, I can't know for
sure how chocolate will affect other people, but Tina and I have
recently discovered (October-November 2011) a causal link between dark
chocolate - or
sufficient quantities of cocoa (including organic raw cacao) - and
RLS/PLMD.
Please let me know your experiences with this.
Most people can consume chocolate without getting RLS/PLMD, but if you
are
predisposed to it for some reason, such as low iron, some inherited
genetic factors or whatever, you may find, as we did, that dark
chocolate or cocoa increases your chances of having RLS/PLMD.
These effects would diminish with time, in part related to the level of
metabolic activity affecting the breakdown and excretion of whatever it
is in chocolate which causes the trouble. I think that having dark
chocolate late at night is likely to be more of a problem than having
it in the afternoon, or morning.
In early November 2011, we went for a 4km walk in the late afternoon
and shared a 100 gram bar of Lindt dark chocolate with roasted
almonds. That night Tina had unusually bad RLS/PLMD.
Without
coffee or any other source of caffeine, on days with little or no
chocolate, she typically has no symptoms at all.
One night she made two chocolate drinks, each with a "tablespoonful"
(actually a desert-spoon) of raw organic
cacao powder
http://www.lovingearth.net/products/12/raw-organic-cacao-powder
. (Cocoa powder is prepared from roasted cacao beans.)
Bad RLS/PLMD followed
that evening. The only other potential contributing factors were
salt, but I think that was not enough to explain what happened.
There have been several other occasions on which raw cacao at night was
followed by unusually bad RLS/PLMD.
Tina's experience with raw cacao makes me think the RLS/PLMD-increasing
effects must be due to something intrinsic to cocoa - not the fats and
other
things which are added to it to create chocolate. I assume it is
not the same mechanism as the
opioid receptor antagonists in coffee, because the 1983 researchers who
found these only found them in coffee, not in chocolate or other common
foodstuffs they tested. (See the coffee section of this website
for more information:
../coffee/
.) These opioid receptor antagonists were not in raw coffee
beans, but were created by the roasting process breaking up molecules
which occur naturally in the beans . Raw cacao hasn't been
roasted, and my impression is that it induces RLS/PLMD symptoms more
strongly than the same quantity of cocoa powder.
Cocoa contains some caffeine and a lot more theobromine, which is like
a caffeine molecule but with a CH
3 group in place of one of
the hydrogens. Theobromine is generally considered to be less
disruptive to the central nervous system (the brain, brain-stem and
spinal cord) than caffeine. Maybe there's something else in cocoa
and chocolate which is causing this RLS/PLMD trouble. I would be
surprised if this amount of trouble was caused just by chocolate's
relatively low caffeine content.
I am much happier without tea, coffee or other forms of caffeine.
I know more than a little dark chocolate will make me anxious and
irritable for a day or two afterwards, and will make me tired and
perhaps give me a headache if I have quite a lot of it for a day or two
and
then stop. However, I
like
chocolate and think its benefits and pleasures in moderation, or
occasional immoderation, outweigh its ill-effects. I ate a little
while writing the Help section, and didn't get RLS/PLMD that night.
I was surprised
to find that dark chocolate and cocoa contributes to the RLS/PLMD that
Tina
and I experience, but that's what we found. I am becoming more
wary of dark chocolate, especially later in the evening.
help07 - Excessive salt seems to worsen or
cause RLS/PLMD
Tina and I have repeatedly observed
that if we eat salty foods, we are more likely to get some RLS/PLMD
symptoms that night. Pizza, salty corn chips and the like,
olives . . . there are quite a few foods and snacks with higher than
average levels of salt. Vegemite (Australia's black
axle-grease-like yeast extract spread) is notoriously salty. I
eat the new half-salt version, which is supposedly for children -
My
First Vegemite. Tina takes her chances with the original full-salt version.
On 16 November 2011 I ate some
salted
cashews before going to bed - this was a bad idea. I had a
few foot movements and some vaguely
restless feet when trying to get to sleep. I used the Homedics
massager (
#help14)
on either side of my spine, from my mid-lower back up to my
shoulders. For good measure I took two 500mg tyrosine capsules
too (
#help13). That fixed the problem.
Google finds lots of pages mentioning salt and RLS. I don't
know
what the mechanisms are but sodium chloride affects blood pressure,
kidney function and many other bodily systems, so it would not be
surprising if it affected something in the spinal cord, especially to
do with circulation or with the transport of amino acids such as
tyrosine across cell membranes. The concentrations of sodium
and chloride ions inside and outside neurons are primary mechanisms
driving their electrical operation. Amino-acid transporter proteins
which span the cell membrane are also affected by these concentrations.
help08
- General nutrition, including Magnesium and Calcium:
Avoiding pernicious drugs - tobacco,
non-prescription opioids, cocaine,
amphatemines, cannabis, etc. is obviously necessary for maintaining
good
health.
Alcohol may bring temporary benefits of aiding sleep and perhaps
(via some indirect generation of opioid receptor agonists) direct
dampening of spinal pain receptor circuitry. However, it is a
carcinogenic (
American Cancer Society)
depressant (
Mayo Clinic) which in the long-term disrupts sleep (
http://www.lmu.edu/Page25070.aspx) - and it has a long
history of causing damage and addiction.
I used to drink wine etc. like most other people, but when I stopped
using
caffeine in 2004, I found I generally didn't feel the need to use it to
relax - which seems to be the primary attraction of
drinking for me and many other people. I might occasionally be tempted by a little wine or a
beer on a really hot day.
Folate (
http://en.wikipedia.org/wiki/Folate
has many references) deficiency is sometimes linked to RLS,
particularly in pregnant women
who may also be short of iron.
http://www.liebertonline.com/..../152460901750269652
Restless Legs Syndrome and Sleep Disturbance during Pregnancy: The Role
of Folate and Iron
Kathryn A. Lee et al. Journal of Women's Health & Gender-Based
Medicine Volume: 10 Issue 4: July 7, 2004:
Compared with those
without complaints of restless legs, those with restless legs had low
serum ferritin at preconception and significantly lower folate levels
during preconception and at each trimester. In addition, time to sleep
onset was significantly delayed and depressed mood was significantly
higher in the RLS group. Rather than indicators of iron deficiency
anemia (serum ferritin, serum iron, and hemoglobin) or pernicious
anemia (vitamin B12), it was reduced serum folate level that was
associated with RLS in this sample of pregnant women.
|
Perhaps most of the folate goes to the developing baby, since it is so
vital for the body building itself. Best to consult your doctor
about
supplements. There's plenty of folate in leafy vegetables.
Folate is vital for may other cellular
processes.
(Note added 2012-04-08.) There's a hypothesis that high levels of
folate in pregnant mothers causes more children to be born with
a genetic disposition to autism.
http://www.ncbi.nlm.nih.gov/pubmed/18514430 http://www.google.com/search?q=folate+autism .
There's considerable debate about vitamin supplements. It seems
that
Vitamin E is no longer
well regarded. It is an anti-oxidant with some possible benefits,
but it also disrupts the body's own oxidative processes for getting
rid of pathogens and errant cells. A 2010 open-access paper in
the British Medical Journal concerning Vitamin E and stroke:
http://www.bmj.com/content/341/bmj.c5702.full
.
The US National Institutes of
Health has information
http://ods.od.nih.gov/factsheets/Zinc-HealthProfessional/
Zinc.
They state that for most adults, 8mg and 40mg are the daily minimum and
maximum allowances, and that vegetarians may need more than the
minimum. Not eating meat (I eat plenty of fish and other seafood),
I take a 25mg Zinc tablet each day, because there is only a small
amount in
the multivitamin tablets we take. A single Zinc atom is essential to the
operation a hundred or so enzymes:
http://lpi.oregonstate.edu/infocenter/minerals/zinc/
.
There are numerous benefits of
Vitamin
D,
including reducing the incidence and progression of many
forms of cancer. These benefits are now being recognised, along
with the need for higher levels than those previously chosen, which
were merely sufficient to prevent the extreme deficiency condition of
rickets. I don't have any evidence for Vitamin D's involvement in
RLS/PLMD, but I mention it because many people are deficient in it
(according to the standards set by recent research, in part due to
people being careful not to expose their skin to the sun), because it
affects many systems within
the body, and because RLS/PLMD symptoms are evidently affected by many
aspects of the body's functioning.
The
Vitamin
D Council http://www.vitamindcouncil.org
has guidance on dosage and having a doctor organize a blood test.
They recommend at least "5,000 IU" for
adults. This may sound like a lot, but "1,000" IU of Vitamin D3
is
25 micrograms: 1/40,000 of a gram. If we took 5,000 IU this for
80 years, it would total
3.65 grams, which is a not-too-heaped teaspoon full.
Many countries still officially adhere to much smaller minimum and
maximum doses
which are out of step with recent research. In Australia, the
biggest Vitamin D3 tablet which can be sold is 2,000 IU. Tina and
I buy small 50,000 IU capsules from the USA:
http://www.biotechpharmacal.com/catalog/category/vitamin-d/
which is less expensive and more convenient than using several locally
available 2,000 IU tablets a day, since we only need one
every ten days or so. ProHealth (
http://www.prohealth.com) sell 50,000 and 25,000 IU capsules. A continually updated compendium of Vitamin D information is:
http://www.vitamindwiki.com .
I understand that a great deal of research indicates that the
Omega 3 fatty acids are very
important for physical and mental health. We take the equivalent of four 1 gram fish oil
capsules a day (two double-strength capsules:
Nature's Way and
Swisse) and eat plenty of fish and other seafood.
Some people find that their RLS problems are reduced or resolved by
taking
Magnesium
supplements. Magnesium and Calcium are generally taken together,
and I understand that proper levels of Vitamin D are essential for
metabolizing Calcium. A number of US manufacturers produce "Cal
Mag Citrate" tablets, for instance:
http://www.jarrow.com/product/79/CalMag . I haven't researched the arguments for the
various forms of Calcium and Magnesium supplementation. I
understand that these supplements and sufficient Vitamin D are well
regarded in terms of reducing the risk of osteoporosis, but the
quantities of Vitamin D in these tablets may be much lower than the
Vitamin D Council recommended daily intake. This analysis and summary of various documents:
www.vitamindwiki.com/...Overview+Magnesium+and+vitamin+D includes material on low levels of magnesium being common in the USA, and that these may impact Vitamin D metabolism.
Further thoughts on nutrition and light exposure to avoid
seasonal affective disorder are on another page:
../coffee/#proper
Light exposure in the morning helps synchronize the circadian rhythm,
which is important for being alert during the day and falling asleep
without trouble in the evening.
[#complexcarbs]
I understand that the sugar addiction work of
Kathleen DesMaisons in New Mexico
http://www.radiantrecovery.com
is highly regarded by many people who have tried it. I read the first five
chapters of the 2008 edition of her memorably named 1998 bestseller
Potatoes not Prozac.
(
Amazon
link) She cites the work of Elliot Blass (Google Scholar
search)
who researched the pain-reducing activation of opioid receptors in rats
due to ingestion of sucrose increasing the production of beta
endorphins. (
Interactions
between sucrose, pain and isolation
distress, 1987 PubMed
abstract.)
These are the same mu opioid receptors which are antagonized by
compounds in coffee.
Some more recent research supports the concept of sugar addiction,
such as this freely available, extensively referenced, 2007 paper:
Evidence for sugar addiction: behavioral
and
neurochemical effects of intermittent, excessive sugar intake,
NM
Aveda et.al, 2008 PubMed
abstract and
full
article.
"The evidence supports the hypothesis that under certain circumstances
rats can become sugar dependent. This may translate to some human
conditions as suggested by the literature on eating disorders and
obesity."
In
#help12 suggest a high-protein snack
before bed may help reduce RLS/PLMD symptoms, but this is contrary to
Kathleen DesMaisons' advice to avoid protein, and instead to consume
complex carbohydrates, such as a potato.
help09 - Avoiding drugs which worsen the
condition
In addition to caffeine, there are a
variety of prescription and non-prescription drugs which may worsen
RLS/PLMD symptoms.
Various SSRIs (Selective Serotonin Re-uptake Inhibitor) and other
antidepressant drugs are reputed to worsen symptoms. Drugs may
have different
effects on different people, and it is possible that some
prescription and non-prescription drugs may reduce the symptoms, at
least
for some people.
One drug I suggest all sufferers steer well clear of is
Phenergan. The chemical name
is
Promethazine http://www.nlm.nih.gov/medlineplus/druginfo/meds/a682284.html
and the drug is sold under a variety of brand names, and as an
antihistamine in cough syrups.
Amongst other effects, Promethazine is a dopamine antagonist: it
occupies dopamine
receptors but does not activate them. This occupation prevents
those receptors from being occupied and activated by dopamine itself,
or by drugs
which also occupy and activate the receptor (dopamine receptor
agonists, such as those frequently used to treat RLS/PLMD).
Phenergan is a CNS (Central Nervous System) depressant, which is
intended to make people drowsy. I understand some parents give it
to their children to calm them down . . . which sounds horrible to
me. (Maybe the children are acting up because they are fed Coca
Cola, Pepsi and excessive sugar and chocolate.)
Tina once took some to help her sleep on the 14 hour flight from Sydney
to Los Angeles. Not only did it make her less sleepy, it set her
RLS/PLMD symptoms on fire for the next two days. In the Yahoo
Groups
RLS Support forum (linked to above
#intro) on
2011-11-11 (message 53522),
there is a report of an injection containing Phenergan leading to
pacing all night with RLS.
I won't try to develop a
list of
medications to avoid. Please refer to the Word file
RLS Medical Alert Card at
http://www.rlshelp.org
which is compiled by RLS-specialist
Mark J. Buchfuhrer M.D . This
lists dozens of drugs
to avoid, with alternatives which cause fewer problems. (If you
don't have Microsoft Word, you can save the file and upload it to
http://view.samurajdata.se -
which will convert and display it in your browser.)
The RLS.org 2010 RLS Medical Bulletin (see
#rlsorgpubs
above) mentions some
medications to avoid (pages 4 and 5), but this is not as extensive as
the RLS Medical Alert Card.
Medications are, ideally, prescribed or suggested for good medical
reasons. So any decision not to take such medications should be
taken in consultation with your doctor or nurse.
help10 - Sleeping position and keeping warm
RLS/PLMD sufferers have probably
figured
out the sleeping positions which worsen or reduce their symptoms.
Tina and I generally find that lying on our backs worsens symptoms.
There's a fascinating chapter (12 Appropriate/Inappropriate Developed
Pain Paths) in the 2009 book "The Science of Pain" (see
#ownresearch below), which I think
is the best reference on spinal nociceptive (pain perception and reflex
generation) circuitry. The author of this chapter, Jens
Schouenborg (
website)
describes how the spinal circuitry for a particular function (in the
case of RLS/PLMD, the foot-withdrawal reflex action and pain perception
in
the dole of the foot) is initially driven by inputs from sensory
neurons all over the body. A pruning process occurs in-utero or
shortly after birth, which would ideally remove all the inputs apart
from those in the particular area of the body which matters.
I propose that these pruning arrangements are imperfect and that
different individuals may have their foot-arch spinal cord circuitry
also driven by sensory neurons from other parts of the body. This
is the best explanation I can give for the observations I am about to
relate.
We have recently discovered some surprising things regarding sleep
position and coolness. I have no idea to what extent this applies
to other people - please let me know your thoughts and experiences:
../contact/ .
At first I thought that the RLS/PLMD-increasing effects we observe of
sleeping on our backs could be due to pressure on the lower back
reducing circulation in
the spinal cord. However, I think the effects of lying on our
backs or on
our sides are too immediate for this to be the primary mechanism.
Also one of our RLS/PLMD-suffering friends finds that her symptoms get
worse if she sleeps on her back.
I now think a more likely explanation is that sensory neurons in
the
skin or flesh of the back are driving the foot-arch spinal
circuitry, due to some imperfect pruning of neuron axons (output terminals) during the development of the
nervous system, before or shortly after birth. So lying on our
back adds input to these circuits,
making them more prone to being triggered by (what I hypothesize is)
the low level of random depolarizations (firing) of sensory
neurons from the skin of the foot arch, even when nothing is touching
the skin there.
Several chapters in "The Science of Pain" note that it is not just
noxious stimuli, such as acute puncturing pressure or heat, which
stimulates the spinal nociceptive circuits. Coldness or even
coolness on some areas of skin can stimulate them as well.
If we consider this in combination with a possibly imperfectly pruned
set of input sensors for the foot-arch protective section of the spinal
cord, then the following observations we have made are more
understandable:
- Cold on the lower back consistently drives RLS/PLMD
symptoms for both
Tina and me. This could be due to cooling down the spinal cord,
but I
think the effects of letting the skin warm up are too immediate for
this to be the full explanation. A hot-water bottle wrapped in a
suitable cloth jacket is a good way of solving this problem.
However I think it would be a bad idea to leave it there for long, or
fall asleep with it there, because of the danger of overheating the
deeper flesh, including the spinal cord.
- Cold
on the mid-back also seems to drive RLS/PLMD symptoms.
Perhaps this and the above observation may be related to the
circulation
shutting down and so reducing the supply of oxygen, glucose, tyrosine
and other nutrients to the spinal cord. I haven't studied
the spinal cord's blood supply, and I guess it would be unrelated to
the skin, but perhaps cooling the skin and deeper flesh does upset
it. One couple reported in a forum message http://earthclinic.com/CURES/restless_legs.html
that they found a menthol cream (which perhaps contains other
ingredients apart from menthol) was generally effective at preventing
RLS/PLMD when rubbed into the lower back. This is most
interesting - but we haven't experimented with it yet.
- Having
a cold or cool upper back can directly drive RLS/PLMD symptoms.
Letting
this area warm up can stop them. There must be other
factors
at work - such as excessive salt, chocolate or cocoa for me, and/or
what I assume is Tina's genetic predisposition to RLS/PLMD - for the
system to be so on
the edge that a small change like this makes the difference between
having or not having Periodic Limb Movements. However I have
observed this in myself and Tina, with
a few minutes warming up or cooling seeming to directly stop or start
the foot movements. On cool or cold nights, when Tina sleeps on
her side, I try to make sure the bedding covers her whole back.
- The same applies to the top and front of the shoulders.
- It
even extends to the forearm being cold! I found this
myself recently (November 2011), lying quite still, with my arm in or
out of the bed. I moved only my arm, and remained still in every
other respect. When my forearm was cool, the PLMD movements
started up within a few minutes. When I tucked it into bed, the skin warmed up and the
PLMD movements stopped within a few minutes. The air was not particularly cold, but
there was
a breeze from a fan which Tina likes by her bedside on warmer
nights. I have also observed this with Tina's forearm being in
the breeze from the fan, or covered up. Neither Tina nor I felt uncomfortable with this coolness. I have repeatedly
observed an apparent causal link with PLMD foot movements apparently
being caused (in part at least) by coolness or coldness of the skin of
the back, shoulders and arms.
help11 - Unusually high or low levels of
exercise
I don't have a specific reference, but
I recall multiple instances in the RLS literature and forum discussion
of researchers and sufferers observing a complex relationship between
exercise and symptoms. Generally, I think, the view is that some
exercise reduces symptoms but too much makes the symptoms worse.
One one or two occasions we have observed a high level of exercise
apparently contributing to RLS/PLMD symptoms that night. An explanation can be found if we consider that a shortage of
tyrosine will reduce the ability of the spinal cord to make dopamine,
especially (or perhaps only, depending on how deficient the blood
tyrosine levels are) when only some of the Tyrosine Hydroxylase enzyme
molecules are working due to a shortage of iron.
When we eat protein, it is broken down into its constituent amino
acids by enzymes in the intestine. The individual amino acid
molecules are transported into the bloodstream. Tyrosine is one
of the larger amino acids. Different food proteins
have different amino acid compositions. The amino acids are
transported around the body in the blood and can be assembled (by huge
enzymes called
ribosomes, according to genetic instructions in messenger RNA) into new
proteins. Some amino acids are also used as precursors for
neurotransmitters. Tyrosine is a precursor for dopamine,
noradrenaline and adrenaline (AKA norepinephrine and
epinephrine). Another large neutral amino acid, tryptophan, is
the precursor for the neurotransmitter serotonin.
If we have an unusually high level of exercise during the day, I
would expect the body to be synthesizing more protein to repair damaged
muscles and perhaps tendons during the night and perhaps for the next few days - and also to make them bigger and stronger
in
readiness for any exercise of this type in the future.
It is not hard to imagine this increased level of protein synthesis
reducing the levels of tyrosine in the blood, so leading to reduced
levels in the Cerebro-Spinal Fluid in the spinal cord, and so to
reduced levels in the
dopaminergic output terminals where tyrosine is needed to produce
dopamine. (These "dopaminergic output terminals" are parts
of the dopamine-producing neurons which release dopamine to reduce the
sensitivity of the soft-touch foot arch reflexes. Dopamine must
be produced in these output terminals on a continual basis.) This
lack of tyrosine my reduce the dopamine production in these output
terminals to the point where they release so little dopamine that it
causes, or contributes to the RLS/PLMD symptoms by failing to
sufficiently inhibit the soft-touch foot arch reflex.
Having too little exercise may constitute "prolonged physical
inactivity" - so during the day the descending dopaminergic output
terminals, which inhibit the foot withdrawal reflex, are depleting
their narrow region of the spinal cord, due to there being insufficient
physical agitation of the cerebro-spinal fluid. This would apply
to many elderly and unwell people, especially anyone confined to bed,
or to a wheelchair.
Also, perhaps excessive inactivity
during the day, with consistently low heart rate and blood flow, may
allow fatty deposits to build up, blocking the
capillaries in the spinal cord where the blood exchanges its nutrients
with the cerebro-spinal fluid. This would reduce the amount of
tyrosine which could be delivered by the blood capillaries to the
Cerebro Spinal Fluid in the spinal cord.
Our bodies are optimized for operation with exercise every day, so it
is
not surprising if things go wrong if we don't get out and walk a
kilometer or two most days.
help12 - Protein meals and snacks
Tina and I have observed a greater
incidence of
RLS/PLMD symptoms if we had a low-protein evening meal, or the meal was
many hours in the past. This would reduce the levels of tyrosine
in the blood. Our biggest fish meals are typically Tasmanian
salmon, and we have observed less RLS/PLMD symptoms on the night of
such meals. The high protein (and therefore tyrosine) content of
the fish is a likely explanation. However, perhaps there are
other factors at work, including the large amount of fish oil.
This points to a simple method of combating RLS/PLMD: high-protein
snacks late at
night. Nuts, maybe cheese, or whatever might be helpful.
However, I suggest avoiding foods which are too salty or hard to
digest. There are various protein powders produced for
body-builders and other people keen to improve their muscle
strength. Many of these are based on whey protein, but soy, peas
and rice protein powders are also available. Some of these list
the amount of tyrosine and other amino acids which are contained in a
single serve.
We often read in bed for a while and an a few occasions Tina has
requested scrambled eggs in bed. On the nights I served her this,
she had no RLS/PLMD symptoms.
I understand that tyrosine can also be synthesized in the liver, from
another similar amino acid: phenylalanine. So perhaps foods with
high levels of these amino acids would be helpful.
While I believe this principle of high protein evening meals and
late-night snacks reducing RLS/PLMD symptoms has a good theoretical
basis and may well be useful for some people, this is at odds with the principle of avoiding high
protein meals late at night, because of the time they take to
digest and the negative impact this can have on sleep.
The next suggestion - taking tyrosine capsules or tablets
before bed,
or during the night if symptoms occur - directly targets the tyrosine
depletion problem without involving proteins or any significant
digestive effort.
help13 - Tyrosine capsules or tablets
The previous section suggested tackling
the tyrosine depletion problem by eating proteins, which are broken
down into their constituent amino acids, one of which is
tyrosine. However, high protein snacks can disrupt sleep.
An alternative, more direct, approach to the problem is to take
tyrosine capsules or tablets before bed,
or during the night if symptoms occur, with half a glass of
water.
There is no digestion required, since there are no proteins to be
broken down. The tyrosine goes straight into the bloodstream
within minutes. We have never noticed any excitatory or
sleep-disturbing effects after ingesting tyrosine. However, this
approach has not been properly researched, and it is possible that some
people may have an adverse reaction to it.
500mg Tyrosine capsules or tablets are
readily available in health-food shops in Australia. As far as I
know, they are a non-prescription nutritional supplement in all
countries. The US chain GNC sells 500mg and 1000mg Tyrosine
capsules or tablets. GNC stores are in many Australian shopping
malls, and Nutralife tyrosine capsules are available in many healthfood
shops. Walmart in the USA carries the Twinlab tyrosine capsules:
Tyrosine powder can also be purchased, for 10 cents a gram or
less.
The formal name for the compound is Levo-Tyrosine (L-Tyrosine) meaning
the left-hand stereoisomer of the molecule. Living things use the
left-hand version of tyrosine and other amino-acids..
We discovered very quickly in 2004 that taking one, two or three
tablets (0.5 to 1.5 grams) would reduce or eliminate RLS/PLMD symptoms,
typically for a few
hours - unless the symptoms were particularly severe (as was sometimes
the case then, primarily due to coffee and/or low iron levels). Other people have
discovered the benefits of oral tyrosine - for instance from 2002:
http://www.rlshelp.org/rlscomp38.htm#L-tyrosine
l-tyrosine is solving my restless legs. I just wanted to get a message to other sufferers.
I have been suffering from RLS for over 20 years and have tried all sorts of cures with no release. Recently I found some info regarding a natural amino acid called L-tyrosine which I have been trying with great success for the past months.
It is truly amazing to stumble upon the answer. Perhaps other RLS sufferers can find similar relief.
to which Dr Buchfuhrer replied:
Various natural remedies such as
L-tyrosine seem to help a small minority of RLS sufferers, but we will
put your information on our web site to see if others may benefit.
|
As far as I know, no-one has formally researched the use of tyrosine
regarding RLS/PLMD. As far as I know, it would only be helpful to
take it at the time the symptoms occurred, rather than taking it during
the day in the hope of cutting down symptoms at night. I imagine that most people who used 500, 1000 or
1500mg of tyrosine at the time of the symptoms would found it helpful - but
without more reports from people who try this, there's no way of
knowing.
I searched the archives of the RLS Support Yahoo Group (see
#forums
above) for "tyrosine", which was mentioned as early as 1999 (msg
4756). One message from late 2000 (15054) reports success using
tyrosine to treat RLS with the effects being apparent within minutes.
Around 2001 it appears some people were trying it, perhaps based on a
recommendation for tyrosine for depression in a 2001 book by Gabriel
Cousens "Depression Free for Life". I haven't seen a copy of
this, but on (2011-11-20) I found an apparent paraphrase of part of the
book
here
.
If your mild
depression and anxiety symptoms during menopause are related to
tyrosine or dopamine imbalance, you may experience relief in as little
as two days, says Cousens.
Some people on the RLS Support forum reported trying tyrosine without
success, but they didn't report their dosage or when they were taking
it. Perhaps some people were taking it during the day,
expecting an overall longer-term positive impact. My
understanding is that oral tyrosine helps reduce RLS/PLMD symptoms for a few hours, and so needs to be
taken when RLS/PLMD symptoms are active or likely to become active. In some other messages,
such as 15559, there are reports of tyrosine being helpful, such as
with one 500mg tablet before bed, another during the night and another
after waking up.
In 2004 I couldn't find any safety warnings about oral tyrosine, so I
took ten
(5 grams) with a glass of water, and didn't notice any effects. A
paper from 1980
Tyrosine for the Treatment of Depression
American Journal of Psychiatry May 1980, 137:5 pages 622-623
Gelenberg, A.J., Wojcik, J.D., Growdon, J.H., Sved, A.F., and Wurtman,
R.J.. Tyrosine for the Treatment of Depression
describes researchers giving a 60kg woman 6 grams (6,000mg) of
tyrosine
a day. This simple treatment consistently resolved her severe
unipolar depression.
On 2011-11-20 I found an excellent resource on the use of tyrosine
supplements for neurological conditions:
This is Chapter 21 of the 2005 book "Nutritional Neuroscience" (
Amazon link). The
chapter is written by
Jan Berend Deijen, of University of
Amsterdam (
his
page)
The chapter concludes:
| Amino
acids used as dietary supplements can interact with prescription drugs
such as monoamine oxidase inhibitors and other antidepressants,
sympathomimetic amines, and opioids (Food and Drug Administration,
1992). |
I also understand that tyrosine supplements may interfere with the
absorption of L-DOPA (Levodopa AKA Sinemet), and that they should not
be taken by anyone with
hyperthyroidism
- an over-active thyroid gland. Tyrosine is commonly recommended
as a supplement for those with hypothyroidism (an underactive thyroid
gland). Tyrosine supplements are not suitable for anyone with one
of the relatively rare disorders known as
Tyrosinemia.
This chapter states that tyrosine supplementation should not be
considered for
pregnant
women, babies or children. Also from this chapter:
The
usual daily L-tyrosine intake from the diet is about 2.2 g for an
individual consuming 100 g protein per day. In one study in which the
extremely high dose of 500 mg/kg body weight (35 g for a 70-kg
individual) was given, no side effects were reported. Thus, from
the information of one subject, L-tyrosine given at ca. 15 times
the
daily intake does not seem to induce side effects. However, as
noted previously, the occurrence of more severe effects of high doses
of L-tyrosine is found in animals receiving low-protein diets.
Therefore, humans with low
intakes of protein may be more susceptible to possible adverse
effects of chronic consumption of L-tyrosine as a dietary supplement.
|
Most of the tyrosine supplementation trials this chapter mentions use
daily doses - either divided or as a single dose - of 100mg/kg body
weight. So for a 70 kg (154lb) person, this is 7 grams - the
equivalent of 14 500mg tablets or capsules.
It is also possible to buy "N-acetyl-tyrosine" supplements. This
has less actual tyrosine per milligram, but is much more soluble in
water. This chapter states that ordinary tyrosine (L-tyrosine) has very limited
solubility in water: 435mg per liter (four cups) at 25C (room
temperature). The research studies mentioned in this chapter used ordinary
tyrosine (L-tyrosine), not N-acetyl-tyrosine.
So as far as I know, two
or three 500mg tyrosine tablets with a glass of water should be generally safe for most healthy adults - but not for
children, pregnant women, or anyone whose health is frail or who has
hyperthyroidism. I suspect
it is probably
safe to do this two or even three times a night. However, I am
not a doctor and I can't advise on the real safety of this, or of any
other drug or nutritional supplement.
We find that 2 or 3 capsules is very helpful in reducing or eliminating
RLS/PLMD symptoms. This can be combined with percussive massage,
as
described below, with the two methods helping each other.
We find that the tyrosine's effects take five to ten minutes to start
and are probably fully established after 20 minutes or so.
This chapter also mentions research which indicates that high levels of
tyrosine in the blood plasma are limited by an upregulation (increased production or activation) in the
liver enzyme tyrosine aminotransferase (TAT), which breaks it down.
It would be great if someone created a sustained release tyrosine
capsule, to release tyrosine into the intestine, and so the blood, over
a period such as 6 to 8 hours. This would provide a
sustained supply of tyrosine all night long. I suspect that only
a small amount is needed per hour, and that taking a gram or so results
in
a sharp peak in the concentration, which diminishes rapidly, such as
within two hours or so.
I think that taking one or two capsules in the event that RLS/PLMD symptoms wakes
the
sufferer up may be quite a useful and sustainable approach, with each
such capsule providing an hour or two's respite.
While we find oral tyrosine and percussive massage very effective, I am not suggesting
them in place of any of the foregoing techniques.
This is why percussive massage and tyrosine
supplements are near the end of this list. While I think
they are likely to be effective and safe for most people, it will
generally be better to avoid direct causes of the problem, such low
iron or opioid receptor antagonists on coffee, than to continue with
such unhealthy arrangements and then try to cope with their impact with
tyrosine and percussive massage.
I hope that by following the suggestions on this list that people will
be able to generally eliminate their symptoms or at least reduce them
to a level which is manageable with tyrosine and percussive massage
(assuming this is actually safe, which I can't say for sure) - rather
than having to use prescription medications such as dopamine agonists
and opioids.
However, Tina and I are not entirely rigid about the above suggestions,
since we
sometimes eat salty
meals or enough dark chocolate to put us at risk of RLS/PLMD
symptoms.
help14 - Percussive massage
First, a caution:
I cannot
assure you that it is safe to use percussive massage on anyone,
especially with a motorized massager. While these devices are
widely used, and may be safe for many people, please make your own
well-informed decisions about how safe this would be for you, such as
by checking first with your doctor or nurse.
In particular I caution against percussive massage for children, the
elderly or infirm, anyone with a back weakness or injury - and pregnant
women.
If you have symptoms in the legs, try performing
percussive
massage
on your mid-lower back, about level with your navel.
Use
your fists or a motorized massager to pummel either side of this part
of your spine
for a minute or
so.
Don't pummel or press
against the bony protrusions of the spine itself - just the ribs and
muscles on either side. This is only for fit and healthy
adults, not for children,
pregnant women, the elderly or anyone with back problems. I can't
assure you that percussive massage is safe for you - you or your doctor
need
to decide whether it is or not.
We find that doing so reduces or
eliminates RLS/PLMD symptoms in the legs, within seconds or a minute or
so. We find that the benefits typically last for hours. I
argue that this is most likely due to the vibration causing renewed
diffusion of tyrosine-rich Cerebro Spinal Fluid into the presumably narrow zone
where the descending dopaminergic output terminals have, over the
previous hours, depleted most of the tyrosine. Within a minute or two, these output
terminals produce more dopamine, typically enough to reduce or
eliminate the disinhibition of the soft-touch foot
arch sensitive circuits, which gave rise to RLS/PLMD symptoms.
If you have symptoms in the upper body (arms) as well, have
someone give you similar percussive massage around your upper spine -
below your neck and between your shoulder blades. As with the
lower back, this needs to be pretty firm to shake the body around a
bit. However, it should not be so hard as to be painful.
Don't pummel or press against the bony
protrusions of the spine itself - just the ribs and
muscles on either side.
I suggest lying face down with your arms lifted forward, so the neck,
upper spinal area and mid spinal area can be massaged without hitting
the shoulder blades.
Tina no longer gets symptoms in the upper
body - she only got symptoms this bad when drinking coffee. (I
suspect several teaspoons of raw cacao just before bedtime might be
enough to induce symptoms so strongly that her arms would be
affected.) When
she did have RLS sensations and PLMD movements in her hands and arms,
we found that this massage of the upper spine would reduce or
eliminate symptoms in the hands and arms, but not the feet and
legs. We found that
percussive massage of the lower spine (around the level of the navel)
would reduce or eliminate
symptoms in the feet and legs but not the hands and arms. I am
confident that the
same observations could be made with any RLS/PLMD sufferer whose
symptoms affect both arms and legs. Any successful etiological
hypothesis needs to explain these observations.
In November 2011, we have two friends who reduce or prevent their
RLS/PLMD
symptoms by using their own fists on their lower backs. These
women are in their fifties and sixties and are in good general
health. You may find this technique helpful, but I can't assure
anyone that percussive massage anywhere on the body is safe. Please
consult your doctor if you have any doubts about the safety of
percussive massage. A forum post in which a husband does
karate-chop-style percussive massage on his wife's lower back is
here: Ginny from Tampa (2011-09-12) at:
http://earthclinic.com/CURES/restless_legs.html
(We have not yet tried her idea of menthol cream on the lower
back. See the help subsection above on sleep position and
coolness of the skin.)
The most likely explanation for the dramatic and localized
effectiveness of percussive massage vibrating the spinal region is that
it quickly diffuses tyrosine-rich Cerebro Spinal Fluid into the tyrosine-depleted
region. However, this massage may also improve circulation in
general, which would help the blood capillaries deliver more tyrosine
in the hours which follow.
If you decide
that this is safe for you, you may like to try it and let
me know what transpires.
../contact/.
For any extensive or regular such massage, I suggest using a motorized
massager with care, if only to avoid Repetitive Strain Injury RSI in
the wrists and arms of the person who would otherwise be doing it
manually. However, the massager body vibrates, so if you use it a
lot, watch out for the vibration affecting sensitive hands and wrists.
We have been happily using this "PA MA" Homedics model since
2005, illustrated below. In early 2012 I found the exact same model at a
Shaver Shop in a nearby shopping mall, though it is not at their website.
We use the rubber domes, rather than the hard plastic ones. This
model has two speeds and heaters, but the heaters are only for
particular hard plastic plastic domes.
The domes are 84mm (3.3") apart. At high speed they vibrate at 45 to 48
Hz with a displacement of about 3.3mm (1/8"). The domes alternate in
their movement. This is ideal for straddling the spine and
strongly vibrating the ribs and muscles on either side of the spine.
Around 2004 Homedics used to make a massager like this where the
business end was in the middle of a large, wide, "U" shaped
handle. It seemed purpose-built for a person to hold it behind
their waist, so the rubber knobs could percussively massage their
mid-lower spinal region. I can't find any such product now.
The above approaches to percussive massage - of the upper spinal and
lower-mid spinal regions - make sense to me in terms of physically
agitating the spinal cord to redistribute the Cerebro Spinal Fluid,
replenishing small parts of the spinal cord where the tyrosine has been
largely depleted by pushing in fresh fluid from a few millimetres
away. This is a very direct method of reversing the lack of
vibration and general physical agitation which results from the
"periods of inactivity" which tend to cause or contribute to the
occurrence of RLS/PLMD symptoms.
#help14_comprehensive_massage
(Added 2012-05-12.) Here is an extended form of percussive
massage - in addition to massaging the areas close to the upper and
lower spine as just described. I call this a
Comprehensive Percussive Massage, although it doesn't concern the front of the body, the hands, lower arms or the head.
We find this even more effective at combating RLS/PLMD than just
massaging the upper and lower spinal areas as described above.
I think this Comprehensive Percussive Massage must help by other
mechanisms than redistributing tyrosine-rich Cerebro Spinal Fluid in
particular parts of the spinal cord. Perhaps it works by
generally increasing circulation - but it does not seem to increase
Tina's heart rate. Perhaps it releases
endorphins
(and other related substances): the body's own (endogenous) opioid
receptor agonists. These would activate opioid receptors, making sleep
more likely and reducing the sensitivity of all the spinal cord's
nociceptive (pain sensing) neurons, including those which drive the
soft-touch foot arch (and palm of the hand) foot (and hand) withdrawal
reflexes.
Perhaps it released endocannabinoids, which are now widely believed to
be the mechanism behind "runner's high", which was previously believed
to result from release of endorphins in response to the pain of
over-exercise. Perhaps this form of massage works by other mechanisms which are not yet understood.
I can't say for sure that this Comprehensive Percussive Massage of most
of the body will help anyone get to sleep or overcome RLS/PLMD.
Nor can I advise whether it is safe for anyone. However we find
it very helpful. Here is how I do it, using the above-illustrated
motorized massager.
- I start by using the massager on either side of the mid-lower spine,
not touching the bony spines of the spine itself which are very close
to the skin. One ball of the massager is to the left of the spine
and the other to the right. I begin at about the level of the navel.
I press quite firmly, such as with a force equivalent to 3 to 5
kilograms (7 to 13 pounds). The instantaneous pressure of the
percussive massage would be greater than this. This is quite a
lot of force, and it is on the borderline of being uncomfortable.
I want to shake the muscles and bones in this area to shake up the
spinal cord, which is fully enclosed by the spine itself. I press
in one pair of spots for five to ten seconds, and then move up or down
to a different pair of spots, in a zone about 15 cm (6 inches) top to
bottom. I do this for 60 to 90 seconds. This action alone
will be quite effective at reducing RLS/PLMD symptoms in Tina's feet
and legs, or on the rare occasions when I have symptoms in my
feet. I do not attempt to move the massager across the skin when
I am pressing so hard. While using the massager on her lower back
with my right hand, I usually smoothly rub Tina's neck and shoulders
with my left hand.
- I then move to the upper spinal region at the base of the neck.
I press quite gently here, moving slowly left and right, and up and
down. I press more firmly on either side of the spine at the top
of the shoulders, but probably only 2 kg or less. I want to shake
up this area as well, just as for the mid-lower spine. I do this
for 60 to 90 seconds too. I use my right hand for the massager,
which leaves my left hand free to smoothly but firmly rub her lower
spinal area. The following steps are the "comprehensive"
extension to this basic percussive massage.
- Next, I move the massager gently from the upper shoulders area, down the mid-spinal area towards
the mid-lower spinal area of step 1. I press gently and move the
massager in a slightly circular fashion as I move it downwards. I
work on this area for a minute or two, quite gently. I speculate
that this improves general circulation in the lower spinal cord.
- For a second time I work on the mid-lower spine, as for step 1, with firm pressure, for a minute or so.
- Now I work on the upper arms.
The two-ball massager is not a good match for this part of the
body. I press gently and keep the massager moving smoothly, from
the shoulder end of the upper arm towards the elbow. I work on
one arm and then the other, avoiding all bony parts. This is
purely massaging the muscle - I am not attempting to vibrate any
bones. I don't know why vibrating the muscle helps, but we find
that all these steps seem to help Tina sleep and avoid RLS/PLMD
symptoms, typically for quite a few hours.
- Next I work on the back and sides of the rib cage in the mid back. I usually start by moving the massager very lightly
over the shoulder blades. Then I press reasonably firmly on the
left side of the spine, below the shoulder blades and down to the
bottom of the rib cage. I move the massager outwards and down the
side of the rib cage. This is really massaging the muscles in
this area, rather than trying to shake up the ribs themselves.
When Tina's RLS/PLMD symptoms were really bad, this part of the massage
would invariably be accompanied by a lot of involuntary kicking!
As far as I can tell, there was no correlation between which side I was
massaging - both legs kicked about as much. This was a perplexing
experience for Tina, but she found it helpful. It is almost as if
I am chasing the heebie-jeebies out of her body with this part of the
massage. The degree of kicking was always in direct proportion to
the severity of her symptoms before the massage began. The kicking did
not resemble the foot withdrawal reflex motion. After a few minutes of
this, the kicking would subside. I do this for a minute or so for
each half of the back, though when her symptoms were so strong as to
elicit kicking, I would spend more time on this part of the massage -
until the kicking subsided.
- I return briefly to the mid-lower spine and then work on the waist and the upper parts of the hips. I press quite firmly and move the massager in various ways, reaching around to the sides of her body.
- Next I massage her bottom and thighs.
Firm pressure and constant movement is the technique here. I am
careful not to get to close to the tendons behind the knees. This
may take several minutes.
- Likewise I massage her calves for a minute or so.
- Before massaging her feet, I return for a final firm session with
her mid-lower back. I may also revisit her neck and shoulder
area. Finally, I massage the bottom of her feet.
This is tricky with the two-ball massager. I press moderately on
the heels, the arch, the ball and the toes. This takes a few
minutes for both feet, and it seems to be well worth spending some time
here. Finally, I turn off the massager and smoothly massage her
calves, feet and each individual toe, two toes at a time.
This takes 10 or 15 minutes. Typically, just before the massage,
Tina would have taken two or so 500mg tyrosine tablets with half a
glass of water.
We find this combination very effective at repelling the RLS monster
and helping her sleep, with the benefits lasting for two or more
hours.
It seems that once she gets enough sleep, perhaps getting enough REM
sleep (which only tends to happen later in the evening once the body's
needs for non-REM sleep are satisfied) that this somehow reduces the
RLS/PLMD mechanisms for the rest of our time in bed. So if the
RLS/PLMD symptoms flare up at 3AM, two tyrosine capsules and a
Comprehensive Full Body Massage will frequently solve the problem for
the rest of the night.
help15 - Other factors and techniques
As some people have written on RLS
forums, we observe that
the menstrual cycle affects the likelihood and severity of RLS/PLMD
symptoms. Trying to research this rigorously would involve
controlling all other factors. I think this would be unethical
to the woman involved and hazardous for the experimenter - who would
need to
stand between his or her premenstrual experimental subject and the chocolate
stash!
Suffice to say that:
- The spinal circuitry can be affected by many aspects of the
body's operation, including the circulatory system and levels of
tyrosine and other amino acids in the blood.
- The menstrual cycle affects and is affected by many bodily
systems.
- It may take only a moderate and otherwise unnoticeable change in one or more bodily systems
to make the difference between no RLS/PLMD symptoms and mild symptoms,
or
between mild symptoms and more severe symptoms.
- Many women towards the end of their menstrual cycle (and perhaps
just
after ovulation) typically crave chocolate - and we find that
chocolate can drive RLS/PLMD symptoms.
No doubt menopause has its effects as well.
Some sufferers have devised exercises which they find reduce or prevent
their symptoms for a significant period of time. This is quite
different from simply walking, or rubbing the soles of the feet - which
brings temporary relief for a few minutes at most.
One fellow did intense push-ups. This would have raised his
heart-rate and probably given his lower back a work-out - both of which
might increase he distribution of tyrosine to the dopaminergic output
terminals in the lower spinal cord.
Other people discovered inverted bicycling helped - hoisting yourself
up on shoulders and elbows, legs in the air, and then moving them as if
pedaling a push-bike. This would be a great way of shaking up the
cerebro-spinal fluid in the spinal cord.
However, this is not the sort of thing most people want to be doing -
or be capable of doing - before going to bed.
[#coffee]
It is best to avoid coffee, including decaf coffee
Further to the sections
#help04 and
#help05
above, please see another section of this website, which is not related
to RLS/PLMD, but concerns the opioid receptor antagonists in
coffee:
This links to all the research papers. As of 2018-11-06 it
also contains a note pointing to research which indicates that coffee,
decaf or not, is likely to be protective against both Parkinsons
disease and Alzheimer's disease, which would constitute a good argument
for drinking it regularly.
2011-10-20 update on
coffee:
A friend of ours also found that
reducing her coffee consumption resulted in a significant decrease in
her RLS symptoms. She was suffering RLS about every third
evening, sometimes in the evening when sitting still, and also when
going to bed or during the night. She has been using percussive
massage on either side of her lower-mid spine (with her own fists) with
considerable success. This would reduce or eliminate the RLS/PLMD
symptoms for hours or for the rest of the night
She was drinking one not-too-strong plunger coffee in the morning, with
one or two not-too-strong instant coffees later in they day. She
also typically had an espresso coffee when she went out, such as once
or twice a week.
In the last few weeks she stopped having these coffees at home and
drank tea instead. She still has one or two coffees a week when
she and her husband go out. She reports that this has
significantly reduced the incidence of RLS/PLMD symptoms.
The history of coffee in England -
and Thomas Willis' observations of RLS/PLMD and on the effects of coffee
Sir Thomas Willis (
Wikipedia
page)
is regarded as the father of clinical neuroscience. He wrote, in
1672 (English translation from the
original Latin) what is
now regarded as the earliest known description of Restless Legs
Syndrome. The following text, or some version of it with
different spellings and typos, is widely quoted:
wherefore
to some, when being a Bed they betake themselves to sleep, presently in the Arms and
Legg Leapings and Contractions of the Tendons, and so great a
Restlessness and Tossings of their Members ensue, that the diseased
are no more able to sleep, than
if they were in a Place of
the greatest Torture.
This is my transcription from
The London
Practice of Physick, Thomas
Willis which can be viewed for free by anyone with a
Google Account, at:
Google digitized this copy from the University of Madrid on 1 October
2010. A fuller quote appears below.
According to this
history of coffee:
http://www.nestleprofessional.com/uk/en/SiteArticles/Pages/History_of_Coffee.aspx
"In the UK, the first coffee house
opened in 1650 in Oxford. The
first London coffee house opened in 1652 in St Michael’s Alley,
Cornhill. Lloyds of London was originally a Coffee Shop called
“Edward Lloyds Coffee House”. London coffee houses were
nicknamed “Penny Universities” because for the price of a cup of
coffee you could sit and join in the stimulating conversation with
the great thinkers of the day. Jonathon’s Coffee House in Change
Alley was frequented by entrepreneurs and merchant venturers,
and was the beginning of the London Stock Exchange. By 1675
there were nearly 3,000 coffee houses in England."
The page
http://www.localhistories.org/population.html
states that the population of England was about 4 million in 1600 and
about 5.5 million in 1700. Interpolating these figures gives a
population of 5.125 million in 1675. If there were in fact 3000
coffee houses, that would be one for every 1708 people.
So it seems that the unfortunate,
"tortured", RLS sufferers Willis observed in 1672 could
have been coffee drinkers. Below I quote Willis writing on
coffee, from the same volume.
In the 2006 book
Restless Legs
Syndrome by Mark J. Buchfuhrer, Wayne A. Hening and Clete A.
Kushida. (Google books
link.)
the authors (p14) state that Cicero (106BC - 43BC) had
the disorder. They also mention as potential RLS sufferers an
earlier and un-named Indian sage, and that French writer Michel de
Montaigne (1533 - 1592) wrote about the restlessness of his legs.
Robert Yoakum's 2006 book of the same name (Amazon Kindle version with
part of the first chapter
link)
has an English translation of the text from Montaigne's final essay
Of Experience, (1587 to 1588,
English translation at
http://equilibrium.org/montaigne/
) in which he mentions his inability to keep his legs still even during
the most interesting church sermons. The passage ends with:
.
. . it may have been said of me from my infancy that I had either folly
or quicksilver in my feet, so much stirring and unsettledness there is
in them, wherever they are placed.
As far as I know, Thomas Willis's report is the earliest recognised
account of RLS/PLMD. What Willis reports is far more intense than
Montaigne's account. His description of torture, leapings and
contractions of tendons, makes me think of one of the videos linked to
above:
k2eGoHk9AAc
Restless
Leg Syndrome? (BF109)
. I know of no suggestion that the disorder was
reported by the physicians of ancient Egypt, India, Greece or
Rome. The above history of coffee begins with:
It
is known that coffee was being
cultivated in the Yemen in the 6th Century AD, though some say it was
drunk as early as 900BC. . . .
Around 900 AD, coffee was well
established in Arabia.
so perhaps these ancient civilizations had little or no really severe
RLS/PLMD because coffee was not used.
My guess is that the symptoms such as reported by Montaigne, from
infancy - inability to keep his legs still while sitting (implicitly
for extended periods of time) - occurs in a small proportion of people
without any involvement of coffee or any other source of
caffeine. There may be genetic, nutritional, developmental or
spinal injury reasons for this. I doubt if the dysfunction which
occurs in these ways reaches the intensity described
by Willis and depicted in the abovementioned video, except perhaps for people with serious spinal
cord damage or other spinal problems.
Willis successfully treated one of his patients with laudanum - a drink
of alcohol with ~10% opium. This is not just my interpretation
of Willis's text - Dr Mark Buchfuhrer and co-authors note on page 15
that he used "laudanum, a preparation of opium". They also wrote
that "we do not know whether a single dose, a short course, or
continued treatment was necessary to control his patient's
symptoms". I guess that at the time they wrote this, there was no
freely available copy of Thomas Willis's book.
Here is my transcription of the relevant passage from Willis, page 404,
concerning what I will refer to as the
RLS/PLMD-style
Watching-Evil. This is from Chapter IV,
Instructions and Prescripts for curing the
Watching Evil and the Watching Coma.
"Watching Evil" means disruption to falling asleep or lack of interest
in doing so, while "Watching Coma"
(p406) means being always inclined to sleep but not being able to do so
properly. I think "Spirits being called from their Watchings"
means
that the person falls asleep, at least temporarily.
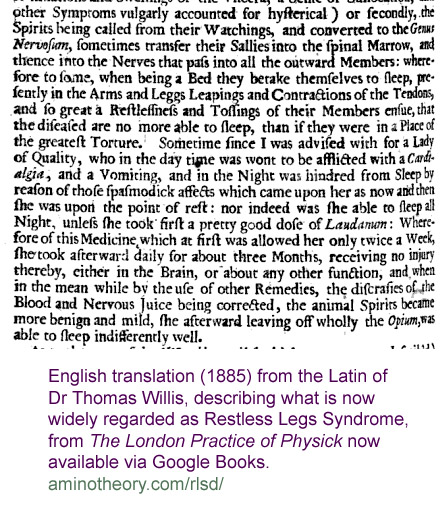
...
or secondly the Spirits being called from their Watchings, and
converted to the Genus Nervosum,
sometimes transfer their Sallies into the spinal Marrow: and thence
into the Nerves that pass into all the outward Members: wherefore
to some, when being a Bed they betake themselves to sleep, presently in the Arms and
Legg Leapings and Contractions of the Tendons, and so great a
Restlessness and Tossings of their Members ensue, that the diseased
are no more able to sleep, than
if they were in a Place of
the greatest Torture.
Sometime since I was advised with for a Lady of Quality, who in the day
time was wont to be afflicted with a Cardialgia,
and a Vomiting, and in the Night was hindred from Sleep by reason of
these spasmodick affects which came upon her as now and then she was
upon the point of rest: nor was she able to sleep all Night, unless she
took first a pretty good dose of Laudanum:
Wherefore of this Medicine, which at first was allowed her only twice a
Week, she took afterward daily for about three Months, receiving no
injury thereby, either in the Brain, or about any other function, and
when in the mean while by the use of other Remedies, the discraises of
the Blood and Nervous Juice being corrected, the animal Spirits became
more benign and mild, she afterward leaving off wholly the Opium, was able to sleep
indifferently well.
So it seems that opium stopped the spasmodic RLS-style Watching-Evil
and enabled her to sleep.
Perhaps
the symptoms were caused largely by coffee, and/or some acute iron
deficiency, and went away a few months after the Lady of Quality
stopped drinking so much coffee and/or improved her nutrition.
The next paragraph, spanning pages 404 and 405, lists various drinks
and preparations for treating the above "RLS/PLMD-style" of
Watching-Evil. Techniques include bleeding ("opening a vein"),
vesicatories (something to do with blistering - Google Books
link)
and opiates. Diacodium is a syrup made from (opium) poppies.
...
moreover let Diacodium and Laudanum, in case they agree well,
be frequently taken; and mean while that the Opiats
give truce from the violence of the Disease, let the cause of it be
eradicated by the use of other Remedies, as much as may be : Wherefore
day after day, at Physical hours, let things be given that take away
the sharpness of the Blood and Nervous Juice, and restore them to
sweetness: In which rank we account Testaceous
Powders (link),
Apozemes
and altering distilled waters of temperate Antiscorbuticks, gentle
preparations of Steel, spirit of Harts-horn, of Soot, and above all
things, tincture of Antimony.
The paragraph which spans pages 405 and 406 concerns a different kind
of Watching-Evil (difficulty attaining or maintaining sleep) than the
presumably RLS kind just mentioned. Sufferers of this kind, which
I will call the "
lack of desire to
sleep" Watching-Evil:
perceive
no drowsiness or heaviness of the Sinciput, no appulse or desire to
sleep. I have known some affected after this manner, who when
they had past many Nights one after the other wholly with out Sleep,
yet being still cheerful and brisk, having a good Stomack, and ready at
business, seemed not as yet to have wanted Sleep.
He likens this to the effects of
coffee:
We may observe that Coffee also on the
same account keeps Persons from Sleeping.
Willis also notes that opiates are unsuitable for inducing sleep (p
406):
Opiats
will not do; for being given in a good large quantity they seldom cause
Sleep, and render the affected more faint and weak. It often
succeeds better if going to bed they take some gentle and pleasant
drink, as especially our being clear and mild, or also posset drink [hot
drink of milk curdled with wine or ale]
with Cowslip Flowers boyled in it, or an emulsion of the Seeds of
Melons and Almonds in great quantity, viz. to two or three pounds.
[#williscoffee]
By the magick of Google Book Search, I was able to find a small
dissertation by Willis on coffee (pp 68-69) - all this is an English
translation of his Latin. The boldface is mine. Willis
identifies two classes of people - one for which he finds coffee
beneficial and the other for which he finds it harmful.
I
shall now say something concerning the Effects of the great
Anti-Hypnotick Coffee.
Coffee, though in some cafes
it be very profitable and Physical, in others it is hurtful and unwholesome ; for we see
that the great Coffee-drinkers
become lean, and are very
often subject to be Parylitick,
and grow impotent for generation.
Yet as to the Affects of the Brain, and of the Genus Nervosum, I very often prescribe this Drink for them.
For indeed in the very many Cephalick Diseases and Infirmaties, viz.
in Head-aches, Giddiness, the Lethargy, Catarrhs, and the like, where
the full habit of Body ; and a cold temperament, or one that is not
hot, and a watery Blood, there is a moist Brain with a sluggishness and
dullness of the Animal Spirits, Coffee often has a very good effect,
for being daily drank, it wonderfully clears and enlightens each part
of the Soul, and disperses all the Clouds of every function.
But on the contrary, those who being thin, and of a Bilious, or
Melancholick temperament, have a sharp or burnt Blood, a hot Brain, and
the Animal Spirits too much stirred and restless, ought to forbear this Drink altogether,
as being apt to pervert both the Spirits and humours in a greater
measure, and to render them wholly
unfit, and unable to perform any functions
: For I have obvserv'd many, not having a sufficient plenty
of Spirits, and also being subject to Head-ache, Vertigo, Palpitation
of the Heart, and a trembling or numbness of the Limbs, who presently
after drinking Coffee became
worse as to those Affects, and suddenly found unusual Langour in their
whole Body.
On pages 415, 418 and 426 he prescribes "a draught of tea or coffee",
which indicates he recognizes a commonality between these two drinks
which we know know as caffeine.
Here are some highly speculative thoughts, hopefully of interest to
history fusspots and the like:
- Willis was aware of coffee and how it affects some people
differently from others.
- The extreme (torture, tossings, writhings) nature of Willis'
description of his page 404 (RLS)
type of Watching-Evil
(insomnia or sleep-disrupting disorder) seems to me to be the sort of
thing which would occur to susceptible people who had been drinking
quite a lot of coffee in recent days. This was characterized by
involuntary limb movements disrupting sleep, rather than a lack of
desire or basic ability to sleep. He finds opiates effective in
treating this condition.
- Willis identifies a second type of Watching-Evil on pages
405-406, which I call the lack of
desire to sleep" Watching-Evil.
While not indicating that this disorder is or could be caused by
coffee, he states that coffee also keeps people from sleeping via the
same mechanisms.
- It is possible for most people to drink coffee and only a subset
get RLS/PLMD symptoms from it, due to the opioid receptor antagonists
it contains and various factors in individual proclivity to RLS/PLMD
symptoms. Some of these people will get very strong symptoms, as
befits Willis's use of "Torture". Because the RLS/PLMD symptoms
may happen many hours to several days after drinking the coffee, and
since coffee in the short term makes them and most other people feel
good, many people will not recognise the connection. This
potentially very strong increase in RLS/PLMD symptoms may occur in a
time-frame where the awakening effects of the caffeine are
insignificant, or later, when the downside of the initial perking up
turns into a lethargy and sleepiness. (I used to fall asleep at
my workbench on quite a few afternoons when I was in my twenties, no
doubt due to the several teas and occasional coffees I drank then.)
- Because coffee was evidently popular in the period in which
Willis was writing, and because he doesn't indicate that these extreme
RLS/PLMD-style symptoms are rare, I wonder if most or all of
the
people he describes with such symptoms were having them largely or
entirely due to drinking coffee. There might be a few who do so
due to spinal injury, but this would be relatively rare.
- Willis observed that opioids (which we now know as opioid
receptor agonists) were an effective treatment for the RLS/PLMD-style
of
Watching-Evil. However he stated that opioids were not suitable
for inducing sleep, including I think, in cases of his "lack of desire
to sleep" Watching-Evil, which was similar to - or perhaps for some
people caused by - the short-term stimulant effects of
coffee. From
this it follows that he recognised that opioids did their beneficial
work on his RLS/PLMD-style Watching-Evil patients by curing the sleep
disruptive sensations and involuntary body movements, not by inducing
sleep in spite of them.
- If
I am correct in thinking that many or all of Willis'
"tortured" sufferers of RLS/PLMD-style Watching-Evil were in fact
coffee
drinkers, then he would have been able to ascertain this pattern by
asking them. Maybe he did, and they were not generally
coffee drinkers, in which case my conjecture is wrong. However,
perhaps he didn't ask, since coffee was widely used and brings on
RLS/PLMD symptoms only for some people. If Willis had discovered
that
his RLS/PLMD-style Watching-Evil sufferers were primarily or solely
coffee
drinkers, then this would have been an important step towards
discovering that coffee contains compounds
which antagonize the effects of opioids. This didn't occur,
and it would be 1983 before some researchers here in Melbourne
discovered this, in vitro, by going on a fishing expedition through
common foods and beverages, looking for compounds with an affinity for
mu opioid receptors in rat brains. If my speculation is true and
if Willis had made this connection, then perhaps
this set of ill-effects of coffee would have been common knowledge for
the last
three centuries.
Coffee puts some people to sleep, and stops RLS/PLMD symptoms - for
an hour or so
Some people find a cup of coffee stops
RLS symptoms and puts them to sleep
On 2011-11-20 two people wrote to the RLS Support forum (
#forums)
in messages 53615 and 53617 that they don't drink much coffee but
sometimes drink a cup of coffee (they did not mention decaf, so I
assume it was
full-caffeine coffee) when they have RLS symptoms, with the effect that
the
symptoms stop for an hour or so, enabling them to get some sleep.
I don't know how much coffee or other sources of caffeine they
use.
This very short-term (minutes to
an hour or so) beneficial effect does not preclude the possibility that
these people are
still suffering a longer-term (days) increase in RLS/PLMD symptoms and
sleep difficulties due to both the caffeine and the opioid receptor
antagonists in coffee.
Perhaps this very short term benefit from coffee is due to the symptoms
being worsened by caffeine withdrawal, and the cup of coffee reversing
those symptoms. (Tina suggested this hypothesis.)
Perhaps the very short-term benefit is caused by the intense caffeine
or some other compounds in the coffee causing a temporary cessation of
symptoms for some reason which is unrelated to withdrawal.
It would be possible to test these two competing hypotheses by having RLS
sufferers who have reported this very short-term benefit from a cup of
coffee having no coffee at all, or any other sources of caffeine, for a
few weeks. Then
if
similar
RLS symptoms appeared, testing to see if the single cup of coffee
stopped the symptoms and helped them sleep for an hour or so.
Assuming
the RLS symptoms appeared, then if the single cup diminished them, this
could not be due to reversing any caffeine withdrawal symptoms which
might have been causing or worsening the RLS symptoms. Another
line of
research would involve these people, with they usual level of caffeine
and coffee usage, taking a caffeine tablet instead of the cup of coffee.
However, I suspect that anyone who drinks coffee and who as RLS/PLMD
symptoms will have less symptoms overall, perhaps no symptoms, when
they stop drinking all coffee,
even
if they consume the same amount of caffeine in other ways.
The logic is simple:
- It is well known that activation of particular spinal opioid receptors reduces or
eliminates RLS/PLMD. (The 32 page PDF version of my hypotheses explains where these receptors are
and why this is the case.)
- Researchers have established beyond reasonable doubt that coffee
of all kinds contains
compounds which antagonize the mu opioid receptors, which are the
primary ones involved in pain/reflex (the same circuits do both)
regulation in the spinal cord.
- Endogenous opioids such as endorphins and enkephalins normally
activate some of these opioid receptors - and so presumably reduce the
levels of RLS/PLMD symptoms below what would occur without this
activation, but the compounds in coffee are known to block such
activation.
The full impact of coffee's opioid receptor antagonists has not been
researched. There may be all sorts of complexities concerning the
various compounds, whose concentrations may vary with different types
of coffee. Different compounds may have different half-lives and
patterns of diffusion in the bloodstream and the CSF in which the brain
and spinal neurons are bathed. Different compounds will have
different
affinities for different types of opioid receptor (mu 1, 2 & 3;
delta 1 & 2; kappa 1, 2 and 3 and the nociceptin receptor).
Perhaps some of these compounds activate some of these receptors, at
least for some people, since there can be genetic differences which
affect the structure and behavior of all these receptors. Perhaps
some
patterns of intermittent or continual activation and/or antagonism will
cause more of some classes of receptor to be expressed, at least in
some parts of the nervous system. Perhaps these actions would
cause
greater generation of endogenous opioids, such as due to antagonism of
auto-receptors which provide negative feedback to the neurons which
release endogenous opioids.
Reducing or halting the ingestion of opioid receptor antagonists might
have a variety of effects. In the long term, we would expect the
previously reduced level of mu receptor activation to return to normal
levels. In the short term, such as days after stopping the
ingestion, it is possible that the levels of activation of mu opioid
receptors would rise above the long-term normal levels, before falling
back to those levels. This could be due to the body readjusting
in various ways.
For instance, exogenous opioid receptor antagonists might be expected
to cause three kinds of short-term adjustments. Sorry I don't
have references handy for any of these - this is from memory from my
neuroscience reading.
- Increase in production of endogenous opioids due to the
antagonists reducing the activity of the autoreceptors on the cells
which produce (or control the production of) the endogenous opioids.
(Autoreceptors in this instance would be activated by opioids and
inhibit the output of the cell - thereby forming a local negative
feedback circuit which would tend to stabilize the production of
opioids, if there were no interference from antagonists.)
- Up-regulation in the number of opioid receptors due to the
antagonists generally reducing their level of activation. I
understand this is a common pattern of adaptation in neuronal systems
in general.
- Perhaps some increase in the sensitivity of individual opioid
receptors, again due to the antagonists reducing their overall level of
activation.
If the antagonists is cleared out of the body (more particularly, out
of the bloodstream and then, with some delays from the CSF in various
parts of the CNS) faster than any of these three adaptive responses
just mentioned, then we might expect a short term increase in opioid
receptor activation, until these adaptive responses were reduced over
the days, weeks or perhaps months which follow.
So any conclusions regarding the impact of drugs or foods in general,
especially regarding caffeine and opioid antagonists such as those in
coffee, should be based on long-term research, no just on what happens
in the days or week after cessation of the ingestion of the substances.
The full impact of these compounds in coffee will take decades to
research. I think they will prove to be important for mood, pain perception and pain
disorders such as fibromyalgia, and for RLS/PLMD.
[#ownresearch]
Conducting your own research
Even if you don't understand anything
about the spinal cord, neurons and neurotransmitters, you can still
experiment with foods, sleeping positions and - if you, or ideally your
doctor, decide it is safe - with oral tyrosine and percussive
massage.
If you report your experiences on one of the forums,
and/or let me know about it, then this will help other sufferers and
their carers. It will also help people who are researching this
disorder.
RLS/PLMD is a neurological disorder. There's nothing wrong with
the skin, muscles or bones in the affected limbs - the problem is that their sensing and control circuits in
the spinal cord are malfunctioning. Food, sleep position and
other potential treatments, including avoidance of disruptive drugs,
all achieve their positive or negative benefits by altering the
function of neurons. So if you experiment with something which
might affect RLS/PLMD and you analyse and report your observations to
others in a clear, scientific, fashion, I would say you are an amateur,
unqualified,
neuroscientist, like me!
Science is an activity. It is not necessary to have formal
training or a degree to do good scientific work.
The scientific process involves carefully observing phenomena,
carefully devising and conducting experiments, and carefully devising
and arguing for and against hypotheses which attempt to elegantly
explain all the known observations. It also involves
imagination, good luck and making the most of mistakes and chance
discoveries.
None of this requires qualifications or academic tenure. However,
it does require patience, education (including self-education) and a
passion for discovering and elegantly explaining Nature.
Even if you don't understand the hypotheses I present, any other
alternative hypotheses, or much about neuroscience, by carefully
observing and experimenting with conditions, foods etc. which affect
RLS/PLMD symptoms - and by sharing these results with others - you can
contribute to neuroscience.
If you have a thirst for knowledge and are familiar with basic
chemistry and biology, you can pursue this in greater depth by learning
more about the nervous system and about RLS/PLMD research.
Unfortunately, many of the research papers are only available via
purchase or access via the library of a university which subscribes to
the publication.
Hands-on research with RLS/PLMD is one of the forefronts of
medical science - it is
probably quite easy to make novel and significant observations, or
devise and conduct new experiments. It is easy to experiment with
foods, sleep
position, massage, coolness of different parts of the body.
The results may show up in less than a day, or even within a
minute. Please let me know what
you find or write about it on the forums listed above
#intro.
I believe that most conventional RLS/PLMD researchers have taken
far too little
interest in exactly what is happening with sufferers and the
discoveries sufferers have made which prevent or reduce their
symptoms.
Its obvious when you
look at the limb movements that they resemble reflex responses. A
few
researchers have noted this, and correctly argued that these responses
are of a purely spinal origin - so it makes sense to look at the spinal
cord, rather than the brain. The most significant paper in this
regard is from 2000:
Also, for background on the particular reflex responses which are being
erroneously triggered in RLS/PLMD, I believe the following article is a crucial
reference for all RLS/PLMD researchers.
Other than citing the above paper, it does not mention RLS/PLMD.
The
lower limb flexion reflex in humans
Giorgio Sandrini, Mariano Serrao, Paolo Rossi, Antonietta Romaniello,
Giorgio Cruccu and Jean Claude Willer.
Progress in Neurobiology. Vol 77, Issue 6, Dec 2005, pp353-395
doi:10.1016/j.pneurobio.2005.11.003
http://unfweb.criugm.qc.ca/jdoyon/cours_6032/Sandrini....pdf
(Freely available.)
Yet I don't recall any RLS/PLMD research papers citing this paper.
Pharmaceutical
companies are primarily interested in funding drug trials - and there
have been dozens of expensive drug trials
for RLS. Tens or hundreds of millions
of dollars are spent each year on prescription medications for RLS, all
of them
with potentially serious side effects. Yet despite all this
effort, none of these researchers have proposed a comprehensive etiological
theory or figured out that
the opioid receptor antagonists which were discovered in coffee in 1983
cause or worsen RLS/PLMD via an easily understandable
mechanism.
There is plenty of scope for amateur neuroscientists
to do
significant new work. Your observations, experiments and
hypotheses may get little or no recognition from mainstream researchers
- but keen researchers can still compare notes and inspire each other's
efforts via Internet communications. If there's a call for it, I
will establish a mailing list for RLS/PLMD researchers - with and without formal training.
Neurology or neuroscience
students
looking for experiments to do as part of their education may also be
interested in conducting research. It is
easy to find experimental subjects. Of the last three electronic
clients who I worked for in Melbourne (November 2011), one suffered
RLS/PLMD himself and
the other two had a parent who suffered from it badly.
In 2012 or 2013, when I have updated my current researcher-only PDF document to
be released publicly, I plan to have a section of this site for
researchers, with a sub-section suggesting experiments for people
studying neurology, neuroscience and sleep medicine.
Assuming you have a basic understanding of chemistry and biology,
it is
pretty easy to pick up some extra neuroscience knowledge from various
Internet sources. Google Scholar and PubMed are particularly
useful:
If you want to develop a broader and deeper understanding of
neuroscience, without spending the next four years at university, I
suggest you buy a textbook and either dip into it, or read it from one
end to the other. It is my impression that neuroscience is the
most complex science of all. The most voluminous textbooks seem
to be neuroscience texts -
and a good neuroscience textbook is beautifully illustrated. In
2004/5 I read what is
perhaps the most prominent of the neuroscience textbooks:
At 1414 pages and 7.4 pounds (over 3kg) this is way too heavy to read
in bed. I cut mine into five comb-bound sections. It is
possible to buy used copies of the 4th edition at
http://www.bookfinder.com for
$60 or so including postage.
I found this a truly fascinating book - but I would not want to be
examined on the vast amount of information it contains. Anyone
looking for insights into higher cognitive or emotional functions is
likely to be disappointed, because most of the brain and most of this
book concerns sensory, motor, visual and
auditory processing. The starting point is neurons and the
proteins and other molecules which make them work, especially the
receptor molecules which sit in the cell membrane of neurons, accepting
molecules which fit into their outside sections and activating a process which changes the internal voltage and so
increases or decreases the chance of it depolarizing (firing) or in some other way alters the function of the neuron.
There are no-doubt other good neuroscience textbooks which are more
up-to-date. In
November 2011, the 5th edition is due in 2013. I suggest not
waiting for this, since this date has been repeatedly pushed
back. The Wikipedia article history shows that in 2006, the 5th
edition was due for release in 2007.
Neuroscience textbooks cover the the brain, spinal cord, muscles and
sensory
neurons, such as in the skin. For RLS/PLMD we need more detailed
information on the spinal nociceptive (pain sensing) circuits, which
are the same circuits which drive reflex muscle movements. As far
as I know, the best
source of up-to-date information in this field is this 1088 page 2008
reference,
which is nearly as hefty as Principles of Neural Science 4th ed.
I read chapters
12, 23, 24, 25, 49 (I read to page 731 and page 734) and 50. I
photocopied the chapters from a library copy.
Reading this formidable volume intently in a train or tram would give
your fellow travelers a fright!
I do not suggest attempting to become an
amateur neurologist.
Neurologists are medical doctors with extensive further training.
They work hard to maintain their knowledge of a vast array of
research and of the clinical experience of their colleagues. They
bring this to bear on your medical
problems in ways which no-one else can. Medical doctors and
neurologists are the only people who can professionally advise you on
the safety or appropriateness of the various treatment options for
RLS/PLMD.
To the index page of this site: ../
Contact details and copyright information: ../contact/
© 2011- 2012 Robin Whittle Melbourne Australia



