Canadian researchers report on their
tests of various components of coffee. They find that
phenylindanes, which are breakdown products of the coffee bean during
roasting, are highly effective in vitro at reducing the aggregation of
of the amyloid beta and tau proteins which, when aggregated, drives the spread and
neurological destruction of Alzheimer's disease (AD)
This, combined with prior research on the apparent protective effects
of coffee regarding AD means that it drinking coffee, decaf or not, may significantly
protect against this terrible neurodegenerative disease.
The initial research was done in 1983
by a team here in Melbourne, Australia. The research was judged
to be significant enough that they were able to publish their initial
paper in
Nature.
J. H.
Boublik, M. J. Quinn, J. A. Clements, A. C. Herington,
K. N. Wynne & J. W. Funder
Coffee contains potent opiate receptor binding activity
Nature 301, 246 - 248 (20 January
1983); doi:10.1038/301246a0
http://www.nature.com/nature/journal/v301/n5897/abs/301246a0.html
(Only the abstract and references are freely available.)
The researchers tested a variety of foodstuffs to find if they
contained any compounds which bound to the mu opioid receptors (MOR) in
rats. This was done by, first of all, exposing the receptors (in a
brain homogenate) to radioactively labeled naloxone, which is a mu
opioid receptor antagonist with a high affinity for the receptor.
When the foodstuff was mixed into the homogenate, the degree to which
any compounds bound to MOR in preference to the naloxone was assayed by measuring how much
radio-labeled naloxone was displaced from the receptors and so went into solution.
The abstract is:
Opiate
receptor-active peptide fragments (exorphins) have been identified
recently in casein and gluten hydrolysates, and morphine has been found
in bovine and human milk. To determine whether similar peptides or
alkaloids occur in other foodstuffs, we have screened potential sources
using a rat brain homogenate assay to detect opiate receptor activity.
We report here that instant coffee powders from a variety of
manufacturers compete with tiitiated naloxone for binding to opiate
receptors in the rat brain membrane preparations, with no significant
difference between normal and decaffeinated coffee. The receptor
binding activity resembles that seen with opiate antagonists, in that
there was no change in the half-maximal effective dose (ED50) in the presence of 100 mM Na+;
on bioassay, the activity was similarly shown to be antagonistic and
specific for opiate-induced inhibition of twitch. Preliminary
characterization of the activity reveals that it has a molecular weight
(MW) in the range 1,000–3,500, is heat-stable, ether-extractable, not
modified by enzymatic digestion with papain, and clearly separable from
caffeine and morphine on TLC. As its concentration in an average cup of
coffee is five times the ED50, these data suggest that
drinking coffee may be followed by effects mediated via opiate
receptors, as well as effects of caffeine.
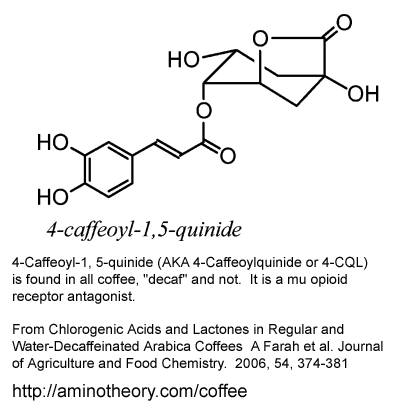
Later research indicates that the most significant of these compounds
appears to be 4-caffeoyl-1, 5-quinide, as illustrated above. This
is according to its affinity for the receptor and its
concentration.
Following the initial paper mentioned above, some of the same
researchers made progress determining which compounds in coffee were
binding to the MOR. They applied for a patent in 1986. I am not
sure about the status of this, but perhaps this is a patent
application rather than an actual patent:
WIPO International Publication Number WO 86/ 01508
Title: Opiate Antagonists
Applicant and inventors:
Commonwealth of Australia c/o The Department of Health, Alexander Building; Phillip, ACT 2606
Kenneth Neville Wynne
Jaroslav Haman Boublik
Olaf Heino Drummer
Ian David Rae
John Watson Funder
http://www.wipo.int/patentscope/search/en/detail.jsf?docId=WO1986001508
("Documents" tab leads to a PDF.)
Abstract:
Compounds of general formula (I), wherein one of the R1, R2 and R3
groups represents a feruloyl or isoferuloyl group of formula (II) or
(III), respectively, and the other R1, R2 and R3 groups represent
hydrogen. These compounds have opiate receptor activity and may be used
in treatment of the toxic effects of opiate narcotic analgesics.
Preparation of these compounds by extraction from coffee, and by
synthetic processes is disclosed.
Some of the team wrote a paper in 1987 (I don't have a copy of this) with more details of the antagonist compounds:
Wynne KN, Familari M, Boublik JH, Drummer OH, Rae ID, Funder JW.
Isolation of opiate receptor ligands in coffee.
Clinical and Experimental Pharmacology and Physiology.
1987 Oct;14(10):785-90.
http://www.ncbi.nlm.nih.gov/pubmed/2832110
I have not done a full literature search on this subject, nor have I
exhaustively read and analyzed these papers, so I have probably not
mentioned some significant papers in the 1990s. The next one is
highly significant, from 2004. It is by a team of researchers at
the Vanderbilt Institute for Coffee Studies:
http://vanderbilt.edu/ics/
Tomas
de Paulis, Patricia Commers, Adriana Farah, Jiali Zhao, Michael P. McDonald, Ruggero Galici, Peter R. Martin.
4-Caffeoyl-1, 5-quinide in roasted coffee inhibits [3H]naloxone
binding and reverses anti-nociceptive effects of morphine in mice
Psychopharmacology (
2004) 176: 146–153
This is available at:
http://vanderbilt.edu/ics/Files/QUINIDE_opioids.pdf
There are other papers on coffee at:
http://vanderbilt.edu/ics/research/ .
The most active compound according to its affinity and concentration is
is "4-Caffeoyl-1, 5-quinide" AKA "4-Caffeoylquinide" AKA "4-CQL"
(Table 1 and page 151). This constituted 0.78% of the coffee
extract. In the conclusion:
In particular, the caffeic acid derivative 4-CQL, which is found in all roasted coffees, showed
in vivo inhibition of morphine-induced anti-nociceptive behavior in
mice with the same order of magnitude as that reported for naloxone.
From the same team, in 2005:
This shows the chemical structure of "4-Caffeoyl-1, 5-quinide" on page 1506. I copied the image into the above graphic.
Also from the same team, in 2006:
This lists (Table 3) the proportion by dry weight of 4-caffeoyl-1,5-quinide
in various coffees. The values are around 1 part per thousand.
There's no new research in this, but in March 2015, the Journal of
Caffeine Research published a letter I wrote concerning these
compounds, the importance of recognising that caffeine is not the only
active compound in coffee, and the impact of these compounds on
Restless Legs Syndrome:
See an update to this regarding caffeine and restless legs syndrome:
../rlsd/briefsumm/#ccc .
This are my thoughts on the likely implications of a large proportion of the population consuming mu opioid
receptor (MOR) antagonists continually, every day, typically for
decades.
The first likely outcome is that the body would up-regulate the
production of endogenous opioids in the bloodstream and/or the
cerebrospinal fluid (CSF). Whatever the complex mechanisms are
behind these background levels, flooding the body with any level
of opioid receptor antagonists would make all the MORs more difficult to
activate. This includes the MORs which (I assume) are located on
the cells which produce the background levels of endogenous
opioids. These are "autoreceptors" which provide local negative
feedback to regulate the cells' endogenous opioid production; likewise the
autoreceptors of the neurons which produce short-term, more localized,
outputs of endogenous opioids.
Endogenous opioids are used in the body both for long-range
communication, where the compounds move large distances from the site
of release to the receptors, and for more synapse-like communication,
where they are released very close to the receptors. These
systems don't have a clear-cut distinction, since any kind of release
of these compounds may cause a general increase in the background
levels, and so affect opioid receptors elsewhere in the body.
I would expect the reduced activation of these
autoreceptors to result in an increased output of endogenous opioids, until the
levels of endogenous opioids became high enough to largely overcome the antagonism due to
the coffee compounds. Likewise, I would expect the neurons which produce
endogenous opioids in a more localized and shorter-term fashion also to produce greater quantities.
If everything were fairly simple, the body would largely adapt to the
continual presence of these MOR antagonists. However the
situation is more complex. There are multiple endogenous
opioids (
http://en.wikipedia.org/wiki/Opioid#Endogenous_opioids),
produced in multiple parts of the central nervous system for various
purposes, with various
physical distributions before they are broken down. The exogenous
(from coffee) MOR antagonists may have varying concentrations in
different locations. There are other kinds of opioid receptors,
although the mu receptors are probably the most important. The
different types of opioid receptor have different affinities for the
various endogenous and exogenous opioids.
Opioid
receptors are located on a variety of neurons which perform a variety of
functions. As far as I know, the research to date shows only that
the exogenous opioid receptor antagonists in coffee effect the mu
opioid receptors. To what extent
the multiple compounds in coffee bind to the other types of opioid
receptors in humans has not been determined. If they do bind,
then it cannot be assumed absolutely that they fail to activate these
opioid receptors.
Update: 2011-09-04: I have only quickly looked at a recently published open-access paper:
Renee N
Donahue, Patricia J McLaughlin and Ian S Zagon
Low-dose naltrexone targets the opioid
growth factor–opioid growth factor receptor pathway to inhibit cell
proliferation: mechanistic evidence from a tissue culture model
Exp. Biol. Med.
2011;236:1036-1050
doi:10.1258/ebm.2011.011121
http://ebm.rsmjournals.com/cgi/content/abstract/236/9/1036
It concerns the body's complex reactions to low doses of the opioid
receptor antagonist naloxone, in particular the differences between
continual and intermittent low doses. Since, as far as I know,
there's no research about the half-life of the MOR antagonists in
coffee, it would be hard to use this research to reliably predict their
effects. (I wrote to the researchers to mention this page.)
One complexity this paper mentions, which I did not initially consider,
is that in addition to raising the levels of endogenous opioid receptor
agonists, there is also likely to be an increase in the number of
opioid receptors. From the first page, with my notes in curly
braces:
The response to opioid antagonist administration is compensatory upregulation in the production of opioid peptides {endogenous opioid receptor agonists} and opioid receptors.
The result of increased numbers of opioid receptors would be similar to
the upregulation in production of endogenous opioid receptor agonists -
more activated opioid receptors than would be the case without these
compensatory changes.
There are many known unknowns:
- The exogenous opioid receptor antagonists in coffee have unknown
half-lives in the blood (serum) and in the CSF (cerebro-spinal fluid,
in which neurons are bathed) in various parts of the CNS (central
nervous system: the brain, brainstem and spinal cord). So we
don't know how long they reduce the activation of opioid receptors for.
- We don't know to what degree they affect different types of opioid receptors.
- We don't know to what degree they cause increased production of
the various types of endogenous opioid receptors in various parts of of
the CNS or how these variations change over time.
- Similarly, we don't know how they affect the upregulation
(increased numbers of) opioid receptors, of various types, in various
parts of the CNS, over varying time periods and according to the dosage.
Nobody knows how many unknown unknowns there are! It would be
difficult to research many of these processes in humans.
Non-human animal experiments would provide some idea of what is
happening in humans, but this wouldn't help with Restless Legs Syndrome
(RLS / PLMS RLSD) because only humans have this condition. Even
if there was a bunch of research about this, it would be difficult to
apply this to an individual, due to variations in genetics, development
and diet.
However, we don't need to wait a decade or two for more research to be
done. All that matters is how coffee affects each individual -
and that is easily determined by using none of it, and no other sources
of caffeine, for a month or two.
I suggest being cautious about coffee substitutes and other kinds of
beverages, including "herbal teas". All these involve infusing a
typically unknown set of compounds into water and ingesting it, which
means most of these compounds go straight into the bloodstream.
Its possible that these drinks also have ill-effects, perhaps similar
to coffee's opioid receptor antagonists, but including any number of
unknown effects.
(End of update.)
There are all
sorts of effects which could arise regarding acute pain perception and
the
threshold of stimulus required for something to be perceived as
pain. Blocking opioid receptors will potentially make us
dysphoric.
The levels of exogenous MOR antagonists will surely vary hour-to-hour
according to coffee consumption. As far as I know, there's no research on
their half-life in the blood or CSF, in rats or humans.
Many or most people drink coffee
several times a week, or several times a day. If so, then their
nervous systems would be continually bathed, probably to a significant extent, in
exogenous mu opioid receptor antagonists.
I used to drink tea, coffee, Coca Cola etc. generally quite
moderately from the age of about 18 to 49. It was a bad idea. I have been consistently happier, more energetic, more
relaxed, less anxious, less irritable, more patient and more
creative since I stopped it altogether in 2004.
Most people think it is normal and unavoidable to feel the way they do,
not least because most people they know feel the same way. Most
people think it is normal to drink alcohol to relax from the inevitable
stresses of daily life. I did. But most of these people are
using caffeine every day.
Hardly anyone thinks that maybe the tea, coffee or whatever is
significantly detracting from their quality of life. Every
morning, they have the experience that a cuppa makes them feel a lot
better than if they didn't have the cuppa. I was the same.
Around 2000 or so
I read of a researcher who, after learning more about the ill effects
of caffeine, went home and eradicated tea, coffee etc. from his house.
I thought that was a bit extreme. Now I understand.
On the assumption that long-term use of coffee will, in general,
antagonize mu opioid receptors more than they are activated by the
likely increase in background (and acutely varying over shorter time
periods) endogenous opioids, here are my thoughts:
RLS / PLMS / RLSD
Later in 2011, I intend this site to have comprehensive material on what I am calling
Restless Limbs Sensorimotor Disorder
because I believe this should be the new name for Restless Legs
Syndrome (RLS) combined with Periodic Limb Movement Syndrome
(PLMS).
RLS/PLMS symptoms are well known to be inhibited by opioids. The
term "opioids" on its own generally means any endogenous compound, or
exogenous synthetic or naturally occurring compound which has an
affinity for opioid receptors and which activates them. A more
precise statement is: RLS/PLMS symptoms are well known to be inhibited
by opioid receptor agonists.
Opioid receptor agonist drugs are widely used to control the symptoms, usually as a
second line or in combination with the first line of defence which are
dopamine receptor agonist drugs. For more information in general
about RLS, see the links at my page
../rlsd/ .
Since opioid receptor agonists prevent or reduce RLS/PLMS symptoms,
we can reasonably expect that exogenous mu opioid receptor (MOR)
antagonists would make RLS/PLMS symptoms worse.
My wife Tina has suffered from RLS/PLMS since she was a child in Texas.
She hasn't been drinking full-strength coffee for a few years.
Her RLS/PLMS was frequently
bad to the point of being
intolerable
when
she did. This year (2011) she firstly reduced her decaf coffee
and later stopped drinking any coffee at all. She has not been
drinking any other caffeinated drinks for several years. Decaf
contains significant caffeine, and caffeine is well known to disturb
sleep and contribute to RLS/PLMS. As noted above, I estimate that
decaf typically has 4% to 6% of the caffeine of regular coffee, but
there would be considerable variation outside this range.
What we observed seems
to result from something beyond the low levels of caffeine which remain in
decaf coffee. I think the effects of three cups of tea a week (a
cup of tea contains about 40mg of coffee, much more than a
typical decaf coffee) probably
would not have contributed so strongly to RLS/PLMS symptoms as the three
decaf coffees.
When she cut back from several decafs a day (two or three, but some were made
with a home percolator and stronger than average) to three a week, her RLS/PLMS
disappeared for about three weeks, and then gradually returned to a
much lower level.
This is all with no caffeinated tea or any other caffeinated drinks -
though she still eats a little chocolate, which contains a small amount
of caffeine and a larger amount of a similar compound, theobromine,
which seems to be much more benign.
A few months later, when she went from three to zero decaf coffees a week, a
similar thing happened: RLS/PLMS disappeared for about a week and
then gradually returned to a still lower level.
Now, her RLS/PLMS problems are a minor and uncommon occurrence, maybe once a week or so.
This is far better than having it most nights. (However, there
were periods in the past when she was drinking coffee when there was
little or no RLS/PLMS, so we are not aware of every variable.)
I think these observations are consistent with my hypothesis that the
continual level of exogenous MOR antagonists due to three decafs a week, or
before that three or so per day, resulted in higher general background levels
of endogenous opioids, but not enough to fully compensate for the
antagonism of whatever opioid receptors are involved in RLS/PLMS.
When Tina cut down to three decafs a week, the exogenous MOR antagonists
suddenly dropped to a fraction of their former level (I am assuming a
half-life such as a day or less). Then her body was still producing, or
at least still had circulating reserves of, a relatively high background level of endogenous
opioids. I guess this would take a few weeks to return to normal
levels.
During those few weeks, I would expect the opioid receptors to be
more
activated than normal (normal = no exogenous MOR antagonists in the
last few months) because the higher than normal, and slowly declining, endogenous opioid level
was not opposed by significant quantities of exogenous MOR
antagonists. So this explains why RLS/PLMS symptoms became
less
prevalent than normal after going from three a day to three a week, and
became less prevalent again after going from three a week to none.
Can anyone report experiences with RLS/PLMS and coffee, especially going from decaf coffee and no other caffeinated drinks to
zero coffee? Is there anyone with severe RLS/PLMS requiring
medication who does not use any caffeine, coffee, or any other drugs
which might contribute to the symptoms? Please let me know:
../contact/ .
Sir Thomas Willis (
Wikipedia page)
wrote, in 1672 (English translation from the original Latin) what is
now regarded as the earliest known description of Restless Legs
Syndrome:
Wherefore to some, when being abed they betake themselves to
sleep, presently in the arms and legs, leapings and contractions
on the tendons, and so great a restlessness and tossings of other
members ensue, that the diseased are no more able to sleep,
than if they were in a place of the greatest torture.
According to:
http://www.nestleprofessional.com/uk/en/SiteArticles/Pages/History_of_Coffee.aspx
"In the UK, the first coffee house opened in 1650 in Oxford. The
first London coffee house opened in 1652 in St Michael’s Alley,
Cornhill. Lloyds of London was originally a Coffee Shop called
“Edward Lloyds Coffee House”. London coffee houses were
nicknamed “Penny Universities” because for the price of a cup of
coffee you could sit and join in the stimulating conversation with
the great thinkers of the day. Jonathon’s Coffee House in Change
Alley was frequented by entrepreneurs and merchant venturers,
and was the beginning of the London Stock Exchange. By 1675
there were nearly 3,000 coffee houses in England."
The page
http://www.localhistories.org/population.html
states that the population of England was about 4 million in 1600 and
about 5.5 million in 1700. Interpolating these figures gives a
population of 5.125 million in 1675. If there were in fact 3000
coffee houses, that would be one for every 1708 people.
So it seems that the unfortunate RLS sufferers Willis observed could have been coffee drinkers.
Anxiety, conflict, irritability and aggression
The NIH already recommends anyone suffering from an anxiety disorder stop using caffeine:
This includes social phobias, any kind of anxiety disorder, especially OCD (Obsessive Compulsive Disorder). Its pretty
obvious that anyone who struggles to contain aggressive impulses should avoid caffeine entirely.
Similarly, anyone with PTSD (Post Traumatic Stress Disorder) shouldn't
be taking any drugs which makes them more anxious. They are
already suffering intrusive thoughts which are typically irrational
reverberations of traumatic experiences in the past. They
re-experience the feeling of helplessness, pain and fear of being annihilated.
Caffeine has been shown to increase the rate of hallucinations in
healthy people who are in a stressful situation. This paper from some researchers at La robe
University, close to where we live:
S.F.
Croce,
J. Bart, S. Callow, J. D’Promontories, J. Dell’Orson, A. Di Clemente,
K. Hanson, M. Valletta, S. Carlota's, B. Ivor's, L. McKenzie, R.
Norman, A. Thieu, M. Mouldered, S. Scapegoat
The effect of caffeine and stress on auditory hallucinations in a non-clinical sample
Personality and Individual Differences 50 (
2011) 626–630
http://www5.ocn.ne.jp/~ajca/cosic23.3-10.pdf
includes in its abstract:
In this study,
92 non-clinical participants were assigned to either a high or a low
stress condition and a high or a low caffeine condition on the basis of
self-report. After they had been primed, the participants were
asked
to listen to white noise and to report each time they heard the song
"White Christmas" during the white noise. The song was never
played. The results indicated that the interaction of stress and
caffeine had a significant effect on the reported frequency of hearing
"White Christmas". The results demonstrated that high caffeine
levels in association with high levels of stressful life events
interacted to produce higher levels of "hallucination" in non-clinical
participants, indicating that further caution needs to be exercised
with the use of this overtly "safe" drug.
Yet counselling services, who routinely see clients with anxiety and
anger problems - and whose relationships are breaking down and riddled with conflict - frequently serve free tea and
coffee, without any health warnings!
Counselors and therapists are probably happy if their clients are only
using caffeine rather than crystal-meth or other illegal drugs.
Still, if there was a way of helping distressed people drink less
caffeine, I believe there would be profound benefits, including lowered
conflict, lowered anxiety and less impetus to drink alcohol, smoke
tobacco or cannabis, or use other drugs in an attempt to quell anxiety.
Many people chose to drink decaf coffee, due to the direct ill-effects
they notice on their sleep from ordinary coffee. However, while
they may think they are getting little or no caffeine, I think the
caffeine they get can still contribute to anxiety, anger, PMS emotional
problems and to a significant worsening of the symptoms of OCD and PTSD.
Ideally, I think, all caffeinated products should come with a health
warning regarding sleep disturbances, anxiety, anger and
nightmares. The NIH advisory on nightmares
http://www.nlm.nih.gov/medlineplus/ency/article/003209.htm states "
Avoid long-term use of tranquilizers, as well as caffeine and other stimulants."
I have had few, if any, really bad nightmares since I stopped using
caffeine and stopped eating chocolate at about 4AM. Getting up in
the middle of the night to each chocolate led to some very interesting
dreams, but some were horrific nightmares. It was bad for my
teeth too.
While decaf coffee will cause less anxiety than ordinary coffee,
ideally everyone should be aware that it still contains significant
caffeine, and that it contains compounds which antagonize opioid
receptors - which can't be good for general happiness and calmness.
I can't imagine that the opioid receptor antagonists in coffee would do
anything but worsen problems with sleep disturbances, irritability, anxiety, aggression
etc. So drinking decaf is not the complete solution to such problems which are caused by regular coffee.
Creativity and happiness vs. dysphoria
When you consider the lengths to which
people will go to get their opioids - endogenous or exogenous - its pretty
obvious that anything which reduces the activation of our opioid receptors
is going to make us less happy, less euphoric, more prone to pain and
sadness etc.
It is not inconceivable that there could be non-linearities and other
complexities which result in the higher levels of endogenous opioids I
postulate above, caused by the autoreceptors being inhibited by the exogenous MOR antagonists in
coffee, somehow leading to happiness, euphoria or some addiction-like
short-term positive outcome for the user. However, for this to be
the case, there would need to be a bunch of opioid receptors involved
in happiness, pain or addictive reward circuits for which the higher
background levels of endogenous opioids would somehow result in higher
activation levels of MOR or other opioid receptors, despite the
presence of the exogenous MOR antagonists. If so, then this might
explain some of the difficulty people have giving up coffee, in
addition to the explanation which flows from caffeine's addictive
properties.
However, overall, I think the exogenous MOR antagonists in coffee
will
generally make people more miserable. If so, then the addictive
nature of coffee, including decaf, would be due to caffeine and
potentially other substances being a stronger
attraction to having another cup than the negative short and medium
term impact of the exogenous MOR antagonists. Since caffeine
results in tiredness, headaches and the like a day or two after
continual ingestion stops, it is easy to see how these withdrawal
effects cause it to be an addictive drug. Another cup makes the
most obvious ill-effects of yesterday's cup(s) go away. Still,
overall, the extra anxiety, irritability, aggressiveness and tiredness
remains.
People's sensitivity to the ill-effects of caffeine varies.
Bigger people and perhaps those with faster metabolisms can probably
drink more of it than people who do not metabolize it quickly for the same level of ill-effects.
Likewise, it is my impression that vigorous exercise immediately after drinking
caffeine will significantly reduce its ill-effects, presumably because
the body breaks it down quickly.
As far as I know caffeine makes everyone more tired, more anxious and probably less creative.
Creativity is hard to measure. There are times when it makes
sense to stay up late and trade-in tomorrow's alertness for
tonight's focussed productivity. I can't rule out overall
benefits arising from the occasional use of caffeine in this
manner. My concern is with people who use it every day.
I did eat some chocolate during the late-night sessions which were part of creating this website!
More
chocolate than I would normally eat in a day. Its worth the
price: some tiredness and extra anxiety in the days which follow.
I find a relatively small amount of chocolate does the trick.
Chocolate contains a little caffeine, quite a lot of the similar
compound theobromine, and no-doubt other psychoactive substances.
Being productive for extended highly focussed periods is only one
aspect of creativity. Having a freely-ranging, relaxed, playful
mind is surely a major part of creatively solving problems, generating
ideas and imagining fantastical scenarios. I find lying in bed
half asleep is a particularly productive time for fresh ideas somehow
floating into my consciousness. The years since 2004 when I quite
caffeine (I never drank decaf coffee) have been more creative and
happier than those before, though a lot of this is due to being happily
married to Tina.
I can't find any research on creativity and caffeine. Fortunately, it is not necessary to rely
on the research of others, since we can quit caffeine, coffee, large
daily doses of chocolate or whatever for a month or so and see what
difference it makes.
Steve Paolina writes about giving up coffee:
http://www.stevepavlina.com/blog/2005/05/how-to-give-up-coffee/
I also feel that caffeine blocks too much of my intuition and
creativity. I miss subtle sensory input, and my thinking becomes too
linear.
Additionally, caffeine definitely disrupts my sleep habits. Even if I
have a cup of coffee in the morning and none for the rest of the day, I
don’t sleep as well. I wake up in the middle of the night, or it’s hard
for me to get out of bed in the morning. When I consume no caffeine, I
sleep more restfully and wake up easily. I also don’t experience so
much midday sleepiness.
In my twenties I used to fall asleep at my desk at work some
afternoons. That was on several cups of tea a day, with
occasional instant and espresso coffee.
It is apparent that many people have a harder time giving up coffee /
caffeine than I did with my two or so scandalously weak cups of tea a
day habit. It is best to taper off the stuff over a
period of days or weeks. Google reports (2011-09-01)
2,050,000 pages for "giving up coffee", with Stave Paolina's page at
number 1.
Amongst other things, caffeine stimulates the brain to respond as if we
are in fight-or-flight mode - as if we are being attacked. Doing
this every day, year-after-year, can't be good.
Still, the hardness and proclivity to push through barriers which
caffeine engenders in our sensibilities may be helpful in some ways
facing the working world, especially if we are working with or
competing with other people who are similarly putting on their coffee /
caffeine armor every day.
Anything which disrupts sleep has got to be bad for creativity.
Coffee does this with caffeine, and depending on how much decaf is
used, this may have enough caffeine to significantly affect
sleep. The opioid receptor antagonists in all coffee can't be
good for sleep either.
Pain management and pain-related disorders such as fibromyalgia
I have never studied these disorders,
but I understand that fibromyalgia is a contentious diagnosis
involving, in part, lower thresholds for what stimulus will be
perceived as pain.
If so, then it would be a bad thing for fibromyalgia suffers to
consume
coffee or any other foodstuff which contains opioid receptor
antagonists - even if the caffeine caused a temporary reduction in the
pain
they feel.
Google (2011-09-01) finds 30.9 million pages for "fibromyalgia". 12.6 million
of them contain the word "coffee"! There are plenty of pages
advising fibromyalgia sufferers to avoid caffeinated beverages, alcohol
and tobacco. There are some pages claiming that it's OK for
fibromyalgia sufferers to drink coffee. I didn't find
anyone reporting that eliminating coffee (and all other caffeinated drinks)
altogether had no beneficial effect on their fibromyalgia symptoms.
Can anyone report their experiences with coffee / caffeine and fibromyalgia? (
../contact/)
Addictions
In this section I am arguing that continual low-level ingestion of
opioid receptor antagonists (such as exist in coffee) will tend to make
people desire or crave the pain-relieving and euphoric aspects of
opioid receptor agonists, while the high level administration of another opioid
receptor antagonist - naltrexone, in
rapid detoxification -
can be helpful for treating any opioid related addictions in people who
want to quit their habit. More information on this use of
naltrexone is at:
The basis for this is that low-levels of opioid antagonists will not
block the activation of opioid receptors by large quantities of
endogenous or exogenous
opioids, whereas such a blockade is achieved with the high "rapid
detoxification" doses of naltrexone. With the high "rapid
detoxification" does of naltrexone, the
person performs the action to
which they are addicted, which generates the endogenous or exogenous
opioid receptor agonists, but does not experience the reinforcing
sensations of happiness, euphoria or pain-relief since naltrexone
molecules are blocking (antagonizing) most of the mu opioid
receptors. I understand
that with a suitably motivated person, this can be an important step in
changing their habitual feelings and behaviors in order to break the
cycle of
addiction.
With low levels of opioid receptor antagonists, I would expect the
person to generally feel less well and less happy - and that large
quantities
of opioid receptor agonist, such as from the following addictive
behaviours, will be experienced, in the short term, as welcome relief
from persistent ill-feeling. The addictive behaviours will
therefore result in pleasure and/or euphoria and so be self-reinforcing.
I plan to expand the following section with proper references as to the
involvement of opioids in the addictive processes of the following
behaviours. The
precise nature of the opioids involved in alcoholism is still a matter
of research and debate:
Regarding high dose naltrexone for treating gambling addition, Google finds plenty of references:
http://www.google.com/search?q=gambling+naltrexone such as:
Morphine, heroin, prescription opiate drugs etc.
There's a long and shocking history of
death, child neglect and abuse, violence, crime and despair from
these highly addictive drugs; not least Britain's attempt to enslave, degrade and kill the Chinese people with opium:
http://en.wikipedia.org/wiki/Opium_wars
. Some great poets, in past centuries at least, have remained creative and productive while smoking opium, but
in general addiction to these drugs is one of humanity's greatest
ongoing disasters.
I think the ill-effects of caffeine and the exogenous MOR antagonists
from coffee would make it harder to feel happy. So I think the
direct hit of smoking, injecting or ingesting large amounts of
exogenous opiates (morphine etc.) would lead not just to pleasure and
euphoria, but to a sense of feeling "normal" as it reversed the
antagonism caused by the coffee compounds.
Surely it would be harder to give up any calming, euphoric, addictive
drug like the opiates if one was feeling more anxious and less euphoric
due to the anxiety caused by caffeine in tea, coffee etc. The
endogenous opioid antagonists in coffee would presumably worsen this
ill-feeling.
Alcohol and alcoholism
Alcoholism is a complex matter, but it
seems that opioids are somehow central to the addiction process.
Naltrexone is an effective drug for treating alcoholism, as part of a
proper treatment program for motivated people. This indicates that alcohol ingestion is somehow leading to the
production of compounds which are opioid receptor agonists and that this is a crucial part of the addictive process.
Even non-addictive drinking could be motivated partially by an attempt
to quell the anxiety and dysphoria which we would expect from continual
use of
caffeine, coffee etc.
While there can be some fun and pleasure drinking, any alcohol
consumption increases the risk of cancer . . . and I have friends dead
or dying from cancer, all of whom have drunk alcohol like most other folk.
Drinking alcohol is a very destructive and indirect method of
activating one's opioid receptors.
Excessive exercise to the point of damage and pain
I know someone who has difficulty
walking due to her obsessive involvement in high-impact aerobics in her thirties.
She permanently damaged her ankles.
I think this sort of addictive behaviour is motivated in part by
the endogenous opioids which result from healthy levels of exercise and
mainly by the higher levels of endogenous opioids the body produces
in response to serious pain. People can become addicted to the
pain-producing behavior causes the production of these endogenous
opioids, just as with shooting up heroin or drinking to excess.
These folks are unwitting (or maybe not so unwitting) masochists.
I think they would be better off with sustainable, non-harmful,
levels of exercise without the lasting damage to their bodies which
typically
occurs from obsessive exercise to and beyond the "pain barrier".
Again, if people are stressed and dysphoric due to caffeine and coffee -
including decaf coffee - I think they are more likely to be
attracted to obsessive exercise, and less likely to be able to give it
up than if they were not imbibing tea, coffee, caffeinated carbonated
drinks etc.
Sex
Sex is basically good. However, to the extent that it becomes an addiction
and
involves destructive relationships or other problems, then it is just
another harmful way of activating our precious opioid
receptors.
Continual ingestion of opioid receptor antagonists as with coffee
would, I think, make people more likely to crave the endogenous opioid
receptor agonists which result from sex - and less likely to be able to
break any habits they develop with this.
Closely related to sex is pursuing erotica / pornography, now available
by the megabyte on the Net. The endogenous opioid involvement in
addiction to this activity is apparent from this paper:
J. Michael Bostwick, Jeffrey A. Gucci
Internet Sex Addiction Treated With Naltrexone
Mayo Colin Kroc. February 2008; 83(2):226-230
http://www.mayoclinicproceedings.com/content/83/2/226.full.pdf
Good sex, especially in a loving relationship, involves feeling relaxed
and trusting, being generous and full of zest . . . and creativity
makes it better still.
Caffeine and coffee are killjoy drugs, making people tired, anxious and at odds with how they need to feel for the best sex.
Pathological gambling
Gambling addiction can be as bad as alcoholism and opiate addiction.
Unlike in most parts of the USA, in Australia most states allow and
encourage poker machines in hotels, as well as lotteries and
betting on horses, dogs, football etc. There are casinos with
hundreds of poker machines - and Blackjack, Craps, Pia Gow, Poker,
Baccarat and Roulette.
The results include family conflict, relationship breakdown,
financial ruin, increased crime and suicide. Regarding the
Crown Casino in Melbourne, in 2009 an Ambulance Employees union
official is
quoted as saying "There's a fairly regular suicide rate there."
Since naltrexone can be an effective tool in helping people overcome
gambling addiction, endogenous opioids clearly play a central role in
this addiction. I think that continually ingesting caffeine and
opioid antagonists in coffee is likely to make people more
attracted to the endogenous opioids produced by gambling - and harder
for them to break the habit.
Other forms of gambling include some uses of the stock market and futures, currencies and commodities trading.
Smoking
Tobacco addition is not regarded as directly involving opioids, since naltrexone is not effective in curbing it.
I think that any drug, such as caffeine, which makes people anxious is
going to increase the temptation to use relaxing (in the short term at
least) drugs such as nicotine. It must be much harder to break a
nicotine habit while taking any anxiogenic drug such as caffeine.
Since coffee contains opioid receptor antagonists, I think the extra pain and
dysphoria which these cause is will be a further barrier to anyone
trying to give up smoking.
Years ago, a friend quit smoking. He started again
because he found himself being very angry and irritable. I recall
he was a coffee drinker, but at the time, it didn't occur to me that
the antisocial tendencies he found so unacceptable in himself when he
quit smoking might have been due to coffee.
Cannabis
The skunk-weed (cannabis with higher THC levels and a different THC to cannabidiol ratio
SciAm reference)
which is very widely used in recent decades seems to be quite different
from the more natural pot which was widely smoked in the 1970s.
I have heard (from social workers) of people who developed very strong
additions to this stuff, and who start the day with a bong or two -
with severe withdrawal symptoms such as vomiting if they don't.
Its my impression that people are smoking skunk-weed to avoid emotional
pain and to relax. They may think this is "getting high", but the
potentially creative "high" of cannabis only occurs if it is used after
not being used for weeks or months. I am not sure if this skunk
weed is capable of creating such a high. The social workers told
me these people are very unstable and unwell. They told me they
would much rather work with heroin addicts, because the cannabis addicts were so unstable.
I don't know what addiction mechanisms are involved, but skunk weed is
evidently far more addictive and psychosis-inducing than whatever the
psychedelic musicians of the late 1960s and early 1970s were smoking.
As with alcohol and tobacco, if people are turning to skunk weed to
escape anxiety and pain, then it would follow that if they used
caffeine, this would increase their anxiety and so perceived need for
the cannabis "high". To the extent that coffee's MOR antagonists
make people feel more dysphoric, anxious and likely to perceive
innocuous sensations as painful, then I expect this would further drive
the desire for the short-term relaxing effects of skunk weed.
Trying to give up an apparently highly addictive drug such as this
would be harder if the smoker was also ingesting opioid receptor
antagonists on a daily basis.
Given the soporific effects of cannabis, it is likely that many people
would turn to caffeinated drinks, including coffee, so they could get
something done.
Seasonal Affective Disorder and Depression
Seasonal Affective Disorder is often
treated with light therapy, to bring the circadian rhythm back into
sync with daytime. It wouldn't be surprising if lack of vitamin D
was contributing to Seasonal Affective Disorder and to depression in
general.
The light which creates vitamin D in our skin is the same UV-B which
gives us sunburn and therefore increases the chance of skin
cancer. So it's not such a good idea to expose the skin to
sunlight during the summer months. There's no way of getting
enough of it in the winter months around latitudes such as Melbourne's
- 37°. The Vitamin D Council
http://www.vitamindcouncil.org
has advice on proper supplementation. The largest tablets allowed
in Australia are 2000 IU, which is perhaps half of what we should be
taking. 50,000 IU tablets are available in the USA: search for
Vitamin D3 Extreme.
Since coffee is the most powerful non-synthetic source of caffeine, it
would not be surprising if many people suffering from depression and
Seasonal Affective Disorder deliberately drink quite a lot of coffee,
believing it is doing them some good, based on the short-term alertness
it brings.
Yet hammering the body with caffeine like this is not going to improve
long-term health. Coffee's opioid receptor antagonists are surely
going to make matters worse, including making it harder to get to sleep.