I wrote this page on 2020-06-22 and
don't have time to keep updating it, such as be trying to mention all
new research and media reports. While the basic concerns about
prisoners' general health, immune system health and COVID-19 infections
remain valid, over time, it will become outdated.
Here are some newer articles of interest, most recent first:
2020-08-09:
2020-08-08:
2020-08-05:
Approximately 10 million people are confined in prisons, jails, correctional centres - hereafter prisons.
They get little sunlight, generally low-grade food and - as far as I
can tell - little or nothing in the way of vitamin and mineral supplements.
COVID-19 spreads rapidly in prisons due to shared toilets and bathrooms and other facilities. Both prisoners and prison staff are at high risk for contracting the disease.
Since prisoner's health is entirely the responsibility of the prison
administrators, and since healthcare costs, and all costs associated
with violence and other crimes in the prison, are borne by the
governments which run the prisons, one would think that it is a
no-brainer to invest a small amount of money in nutritional supplements
to improve prisoners' health.
Yet it seems that in general, prisoners only get the vitamin
supplements they buy for themselves, with their limited spending money.
Some of the most important COVID-19 statistics for any population are:
- Total number of people.
- Number of people infected so far. This can only be known
with extensive testing and reliable antibody tests - and this is rarely
done.
- Number of people tested positive for SARS-CoV-RNA.
- Number of people tested for this.
- Number of deaths attributed to COVID-19.
- The ages and comorbidities of the people who died.
We are also concerned about the lasting harm done to those who survive
severe COVID-19 symptoms. This is much harder to define or
measure, but I guess that for every person who dies, three to ten
survive with lasting harm, such as neurological damage (micro-embolisms
and on a larger scale, stroke) and damage to their eyes, heart, lungs,
liver and kidneys.
The current death toll is the tip of the iceberg. Firstly,
because if new infections stopped today, many more people will die in
the month to several months following their initial infection.
Secondly, because the number of people seriously harmed surely scales
with the number of deaths.
I have not tried to research this assiduously. The arguments above - in the context of the research articles I link to at
../cv19/ and
../cv19/icu/ - all that anyone should need.
The Marshal Project tracks COVID-19 deaths in US prisons:
https://www.themarshallproject.org/2020/05/01/a-state-by-state-look-at-coronavirus-in-prisons
Here are some "at least" figures from their 2020-06-12 update:
43,967 cases.
These are prisoners who tested positive for viral RNA, meaning they have
been infected recently and may be infected at the time of the
test. As a proportion of the prison population (2.3 million) this
is
1.9%.
In the whole US population 331 million (including prisoners), 2,263,749 people have tested positive = 0.68%.
The states with the greatest number of cases are these, with the
percentage of prisoners who have tested positive, followed by numbers
of tests per 10,000 prisoners. (This is not the same as the
number of prisoners tested, since some may be tested two or more times.)
Texas 6,998 5.0% 6,915
Federal 6,394 3.7% -
Ohio 4,858 10.0% 2,366
Michigan 3,948 10.5% 10,082
Tennessee 3,028 2.6% -
New Jersey 2,451 13.6% -
On this basis, prisoners are getting COVID-19 at 2.8 times the rate of
the whole population. It is possible that some of this explained
by greater depth of testing within prisons than within the rest of the
population, but I think it is reasonable to think that the real rate of
infections in prisons is higher then in the rest of the country.
Each state's entry in the above page shows the known cases, deaths and
(if known) the number of tests, together with how this compares for
these figures for the state overall.
522 deaths. This is
0.023% of the prison population and
1.18% of the total known cases. Total US deaths so far have been 120,688 / 331,000,000 =
0.036% of the population and 120,688 / 2,263,749 =
5.3% of total known cases.
Taking the four states with the greatest number of deaths per
million people - New York, New Jersey, Connecticut and Massachusetts -
in these there is an average of 0.134% of the population killed by
COVID-19.
Most people killed - and I guess seriously harmed - by COVID-19 in the
general population are over 60 years old. However, very few
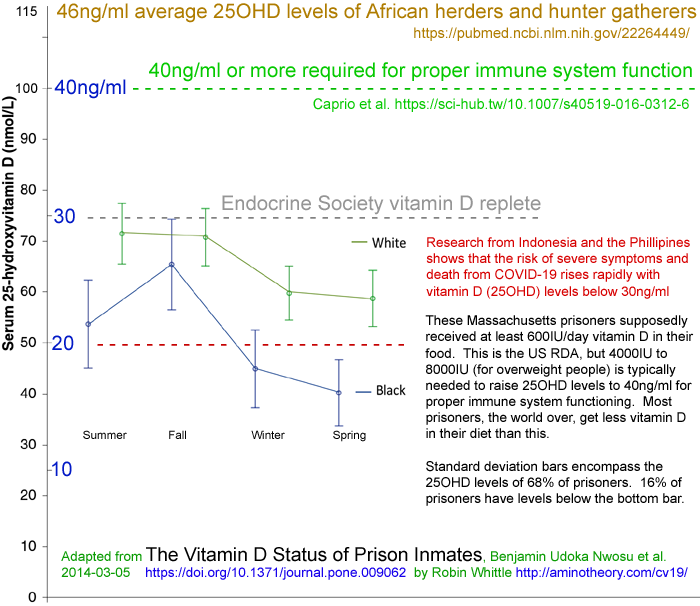
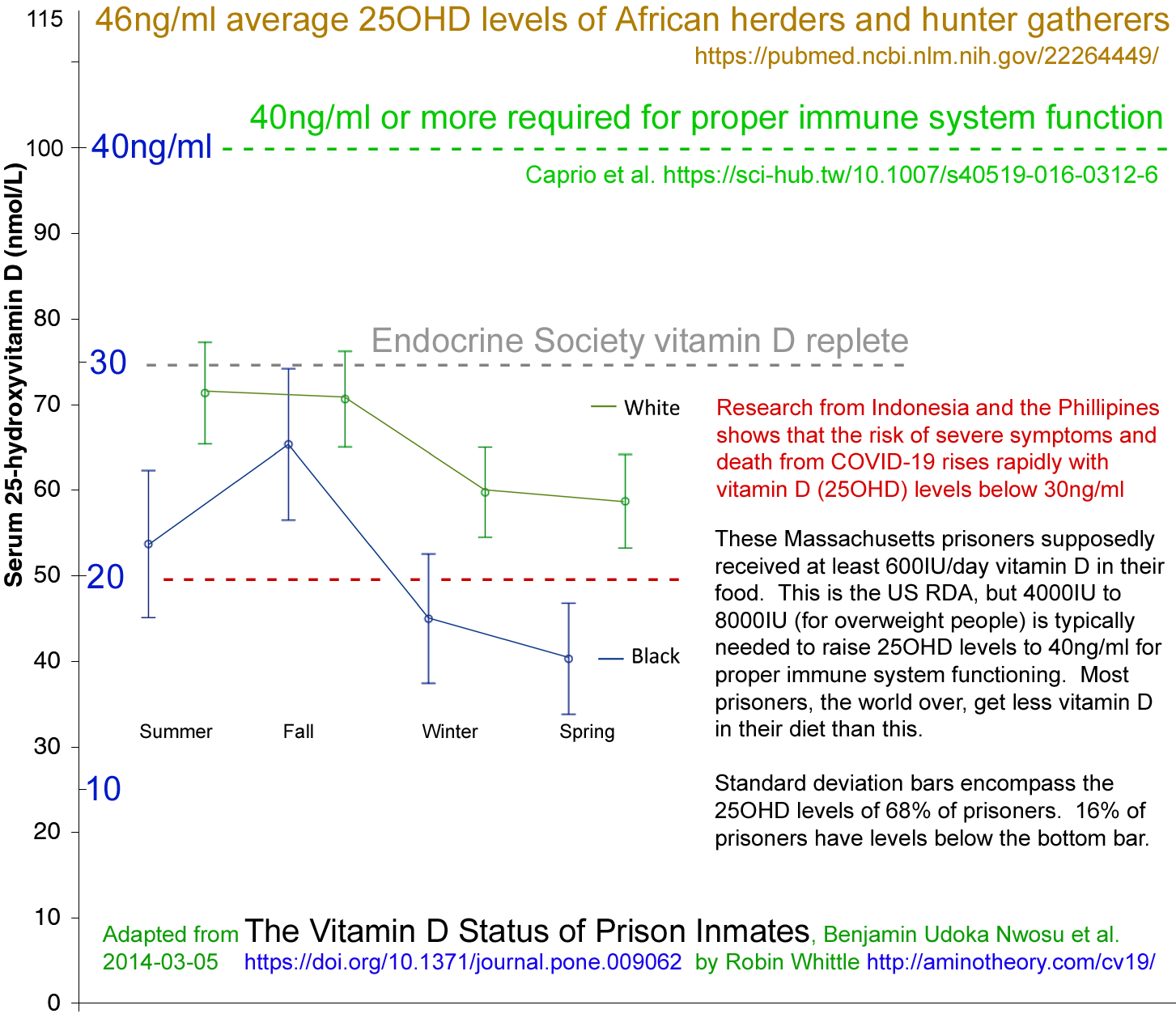
incarcerated people are this old. The average age of the
Massachusetts inmates was 49 for men and 44 for women.
Here is the only bar graph I could easily find, from
https://sites.google.com/site/generationalincarceration/

However, the proportion of US prisoners aged 55+ has increased since 2011. This page has some data from 2015 and 2016:
https://www.pewtrusts.org/.../articles/2018/02/20/aging-prison-populations-drive-up-costs
I did not find any age data on the COVID-19 deaths of prisoners. In the general population, a graph from
Ohio with figures up to 2020--05-19 shows deaths as a percentage of confirmed cases in 7 adult decades:
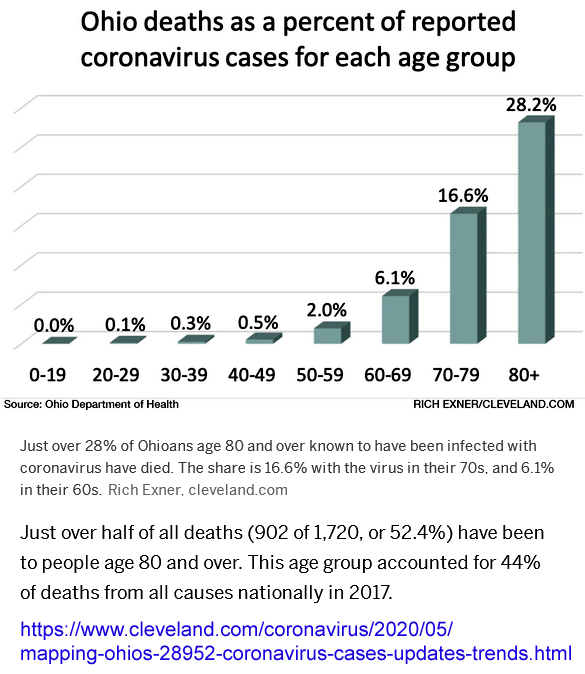
It is
possible that almost all
of the incarcerated people killed by COVID-19 are over 50, but my guess
is that these trends are important:
- The death rate as a percentage of population 0.023% is somewhat lower in prisons than in the general population 0.036%
primarily due to there being few people in the 60+ age range in
prison. It is also possible that the infections there have been
somewhat delayed compared to those on the outside.
- The same could be said of the death rate per confirmed cases, but an additional factor in this being lower in prison 1.18% than in the wider community 5.3%
is that the number of tests done per 10,000 people in prison is
significantly higher than in the general population. In other
words, the number of confirmed cases in prison is closer to the real number of
infections than it is in the community.
So the real question of interest - deaths per number of people infected
- can't be answered reliably, but if the community
had been tested as well as the prisons, the community rate would be lower than 5.3% and so closer to the deaths per number of people actually infected.
- With more thorough testing, including of asymptomatic people,
early treatment and effective isolation, prisons may have been able to
slow transmission and reduce the rates of serious infection
considerably compared to what would have happened if there had been no
such testing or further actions.
I guess that a much greater proportion of asymptomatic people were
tested in prisons than in the wider community - where it was frequently
difficult to get tested due to the need for travel, eligibility
requirements involving active symptoms, or known exposure, and the high
cost of the tests themselves, for some people at least.
- While I can't directly infer this from the above data, I suspect that the average age of death from COVID-19 among incarcerated
people is lower than that in the wider community by several
decades. Therefore, even if (for a
variety of health and behavioural reasons) the incarcerated people on
average have a lower life expectancy than non-incarcerated people they are still, as a group,
suffering a greater loss of life years per individual killed than, on
average, those generally older people in the community who died.
- Assuming point 4 is true - COVID-19 is killing prisoners younger
than in those it kills in the general community - then the same pattern
is surely true of the people it seriously harms.
For simplicity I wrote as if COVID-19 kills and harms people. See the main pages here
../cv19/
for why this is not true. COVID-19 is the illness caused by the
SARS-CoV-2 virus. For people with strong, well-regulated, immune
systems, there may be few or no symptoms and little risk of harm or
death. Generally, those harmed and killed are those whose
weakened and dysregulated immune systems firstly fail to fight off the
virus and then go into over-inflammatory, self-destructive, overdrive -
and it is this which causes the severe symptoms, lasting harm and
death. I and a growing number of doctors and lay people believe that Inadequate vitamin D is the biggest single easily
correctable cause of these immune system failures.
The Marshall Project also reported that
among prison staff there are 9,180 known cases and 38 deaths.
This data is incomplete. In this Guardian
account of
Last Week Tonight's John Oliver's 2020-06-21
video
on COVID-19 in prisons, mentioned more than 68,000 US prisoners (of 2.2
million) known to have COVID-19 and that there are 455,000 staff.
This story also linked to a Marshall Project
page which states that about 200,000 people enter and leave US jails every week.
The general population needs vitamin D supplementation, for numerous reasons - most urgently COVID-19.
The same is true of prison staff, who are generally at higher risk than
most people in the community, because of the nature of their
work. They can afford and easily use vitamin supplements,
including vitamin D supplements.
The same is true of prisoners - but they cannot easily buy their own
supplements - and they are at high risk of infection, with their
extremely limited behavioural choices, close living conditions with
shared facilities, low vitamin D levels and limited access to
high-elevation sunshine.
522 incarcerated people and at least 38 prison staff are now dead from
COVID-19. I believe that few, if any, of them would have been
killed if their vitamin D levels were 40ng/ml or more.
A much greater number of these people have suffered lasting harm for the same reason.
Robust vitamin D supplementation is vastly easier, safer and cheaper than all this.
In the general population it is tricky to encourage most people to buy and take supplements.
I imagine it would be much easier in a prison. The supplements
can be purchased in bulk, at wholesale prices. They can be
distributed with little trouble to the prison population.
Improvements to general health would reduce health and other costs far
more than the cost of the supplements. All this has always been
true. COVID-19 makes it a matter of extreme urgency that such
supplementation programs begin immediately.
None of these people were on death row. But now they are dead and
a greater number have brain damage, kidney damage etc.
There may be some profound problems sourcing vitamin D in the quantities
needed for supplementing the whole population in the weeks and months
to come. So increased exposure to high-elevation sunlight should
be maximised.
Please see other pages at this site, linked to from the main page
../
for notes on the optimal - generally amount of sun or UVB exposure for
generating vitamin D while minimising DNA damage and therefore risk of
skin cancer.
I think there may also be a case for exposure to
artificial UVB light
- though this involves some risk of cancerous skin damage, and the need
to protect the eyes. Another page
../crisis-diy/
(not ready yet) will explore artificial UVB light exposure and
alternative sources of vitamin D if the pharmaceutical stocks have been
exhausted.
{kind=link}